CHAPTER 105 Tropical Diarrhea and Malabsorption
Diarrhea and malabsorption are common in the tropics and most often result from infectious causes. Enteric infections that cause diarrhea are common in tropical countries, a result both of deficient sanitation and the ambient temperature that fosters proliferation of infectious organisms in water and food. Tropical diarrhea affects not only the indigenous population but also visitors to the tropics,1 who are more susceptible than residents to symptomatic enteric infection and who commonly develop diarrhea either during or shortly after their visit.
It has been shown repeatedly that a significant number of asymptomatic and apparently healthy residents in the tropics transiently harbor pathogenic microbes in their gastrointestinal tracts. Up to 15% of the rural population in some countries is infected at any given time by a variety of pathogens, such as Campylobacter, Cryptosporidium, and Giardia species.2–4 By and large, however, a homeostasis is achieved that is perturbed when the person is infected with an overwhelming number of pathogens or when there is impairment of intestinal immunity; this results in diarrheal illness. Residents of the tropics, possibly by virtue of repeated exposure to these or related pathogens, remain asymptomatic, whereas visitors to the tropics quickly develop symptoms upon exposure.
The predominant cause of malabsorption varies with geographic location in the tropics.5–7 In many areas, tropical sprue remains the major cause of malabsorption in adults and a lesser cause of malabsorption in children. Parasitic infections of the small intestine are probably the next most common cause of chronic diarrhea and malabsorption in many areas. In belts of the tropics, celiac disease is now becoming an increasingly diagnosed and appreciated problem and needs to be considered in the differential diagnosis of malabsorption. Intestinal tuberculosis, small intestinal bacterial overgrowth, and pancreatic steatorrhea are other significant causes of malabsorption in the tropics. This chapter deals mainly with tropical sprue and tropical enteropathy, but it discusses very briefly other specific causes of diarrhea and malabsorption in the tropics.
INFECTIOUS DIARRHEA IN THE TROPICS
Acute and chronic infectious diarrhea in the tropics is caused by a variety of bacterial, viral, and parasitic agents (Table 105-1). Although these pathogens affect the indigenous population of the tropics, many of these infected persons remain asymptomatic, probably because of immunity acquired by earlier exposures to the same or related infectious agents. The risk of diarrhea in visitors to the tropics can range up to 55%, depending on their specific travel destination.8
Table 105-1 Causes of Infectious Diarrhea in the Tropics
Cholera is the most dramatic form of acute diarrhea, resulting in death from dehydration and electrolyte imbalance, if untreated. The disease occurs in both endemic and epidemic form in the tropics and mainly affects the indigenous population. Only very occasionally does cholera afflict Western travelers.9,10 Cholera is endemic in the Indian subcontinent, particularly in the southern and eastern parts; in the Indonesian islands; in the Philippines; and also in Latin America.
In a study of 17,353 returned travelers from tropical countries, acute diarrhea occurred in 22.2% and chronic diarrhea in 11.3%.9 Parasitic diarrhea (giardiasis and amebiasis) was most common overall, whereas bacterial diarrhea (Campylobacter > Shigella > nontyphoidal Salmonella) was more common in travelers to Southeast Asian countries. Diarrhea in travelers is often geographically determined, being caused by enterotoxin-producing Escherichia coli with travel to South America or to Mexico, by Giardia lamblia and Cryptosporidium in southern Central Asia, and by Campylobacter in Southeast Asia.9,11 Infection with the coccidian parasites occasionally causes diarrhea in travelers to the tropics. Cyclospora cayetanensis first was reported to cause outbreaks and prolonged diarrhea in travelers to Nepal and has subsequently been reported from other regions in the tropics including Southeast Asia, Africa, Turkey, and Latin America.12,13 Blastocystis hominis is another opportunistic protozoan that occasionally causes acute or chronic diarrhea in travelers.14
TROPICAL SPRUE
Tropical sprue remains a significant cause of malabsorption in several tropical countries. The etiology of this disease continues to remain obscure, and it is unlikely that it will ever be conclusively settled given its diminishing presence. Tropical sprue needs to be differentiated from a variety of other conditions that also cause malabsorption in residents of the tropics (Table 105-2).
Table 105-2 Causes of Malabsorption Syndrome in the Tropics
HIV, human immunodeficiency virus.
DEFINITION
Tropical sprue is a primary (i.e., not caused by other known disease) malabsorption syndrome that occurs in visitors to or residents of the tropics. Baker and Klipstein,15 working in South India and Central America respectively, defined tropical sprue as an intestinal mucosal disease characterized by malabsorption of two or more unrelated nutrient groups (e.g., fat, carbohydrate, vitamins) where other known causes of malabsorption had been excluded. Historically, this definition originated at a time when testing for intestinal absorption was commonplace. The availability of specific diagnostic tests for many of the diseases that cause malabsorption, such as abdominal imaging for chronic pancreatitis or antiendomysial and antitissue transglutaminase antibody for celiac disease, led to a general decline in the use of tests for absorption. In the developed world it is now uncommon to find laboratories that perform tests for absorption, particularly fecal fat estimation.16 The diagnosis of tropical sprue, however, continues to require the demonstration of malabsorption and the exclusion of other specific pathologies including celiac disease, chronic pancreatitis, and parasitic infections.
HISTORY
Modern medical history records the first description of tropical sprue from Barbados in the West Indies by William Hillary in 1759.17 He described this disease (aphthoides chronica) as commencing with severe mouth ulcers and glossitis, followed sequentially by diarrhea, marasmus, and death. The word sprue probably originated from the Dutch term sprouw used to describe a condition characterized by severe aphthous ulceration of the mouth and stomatitis.18 The Dutch used the term Indische Sprouw to describe what appeared to be the same condition occurring in their colonies in Southeast Asia. A similar illness was noted in Europeans who spent time in the Asian colonies including India, Indochina, and China and that went by many names including “chronic diarrhea of the tropics” before being named “sprue” by Manson in 1880.17 Although now primarily described in Westerners who have spent some time in the tropics, descriptions of a malabsorption syndrome in the indigenous population in India date back to the second century bc. The ancient Indian medical textbook the Charaka Samhita19 described an illness (Grahani vyadhi) characterized by glossitis, diarrhea, malabsorption-like stools, and wasting and ascribed to a loss of the digestive fire.
EPIDEMIOLOGY
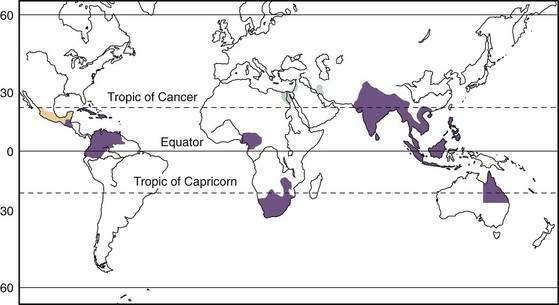
Tropical sprue has been described in South and Southeast Asia, Central America, South America, the Caribbean islands, and parts of Africa (Fig. 105-1). Endemic tropical sprue is most often recognized in visitors who have spent at least a few months in the tropics before returning home,20–22 although tropical sprue or tropical malabsorption also occurs in indigenous residents of the tropics.23–26 It is not clear, however, if the disease that occurs in returning Westerners is the same as the one that occurs in indigenous residents of the tropics. At least in expatriates returning to Europe, it appears that that tropical sprue may be secondary to prolonged infection, or follows an unusual infection, an occurrence that has been called postinfectious malabsorption.27
Tropical sprue also has occurred in epidemic form.5 Epidemics occurred in soldiers and prisoners of war in Asia during the Second World War28,29 and also were reported in South India during the 1960s and 1970s.30 Epidemic tropical sprue affected adults more often than it did children, and exposure during the first wave of an epidemic often conferred protection during the second wave; intrafamilial secondary transmission of disease also was noted. In the early 1960s, epidemic sprue was responsible for the deaths of 30,000 to 40,000 people in South India alone. A seasonal occurrence of tropical sprue was noted in Puerto Rico, where it was common during the first three months of the year.31
Epidemic sprue is no longer reported from South India or other parts of the world. Sporadic tropical sprue also has become relatively rare in some areas of India,7 compared with celiac disease and intestinal tuberculosis, where it once used to represent the major cause of malabsorption and chronic diarrhea. Nonetheless, tropical sprue continues to account for a significant proportion of adult malabsorption and a smaller proportion of childhood malabsorption in South Asia.6,24,25
ETIOLOGY
The etiology of tropical sprue remains unknown. Persistent infection of the small intestine with coliform organisms was postulated to cause the disease in some areas of the world. In Haiti and Puerto Rico, overgrowth of toxin-producing coliforms (Klebsiella spp., Enterobacter cloacae, or E. coli) in the small bowel was associated with feasting and ingesting excessive amounts of long-chain unsaturated fatty acids.32,33 Bacterial overgrowth in the proximal small intestine in patients with tropical sprue also has been noted in other parts of the world, but it has been ascribed to the slow small intestinal transit that characterizes the disease.34 The normal human jejunum contains up to 103 bacteria per milliliter of luminal fluid in Western residents, and bacterial overgrowth is considered to occur when the concentration of bacteria exceeds 105/mL. These criteria, however, do not necessarily hold true for apparently healthy residents of the tropics, and studies in South India have demonstrated that bacterial counts in jejunal luminal fluid ranged up to 105/mL in healthy asymptomatic persons.35 Patients with tropical sprue and asymptomatic persons from the same backgrounds had similar levels and types of bacteria in their proximal small intestine, indicating that bacterial overgrowth probably was not responsible for the malabsorption of tropical sprue. Toxin-producing bacteria were not found in the intestine of patients with tropical sprue in South India.36
Viral particles resembling human enteric coronaviruses have been identified in the stool and jejunal enterocytes of patients with tropical sprue,37 but they also may be present in apparently normal persons, so they have not been definitely implicated in the etiology of sprue. Acute and reversible flattening of the small intestinal mucosa identical to that seen with tropical sprue has been noted in the absence of gluten-sensitive enteropathy and ascribed to a probable viral etiology.38
CLINICAL FEATURES
Although tropical sprue does occur in children, typically the disease affects adults. Presentation is with chronic diarrhea, steatorrhea, glossitis, abdominal distention, prominent bowel sounds or borborygmi, and weight loss (Table 105-3). In expatriates and during epidemics, the illness often begins with fever and watery or, rarely, bloody diarrhea. These symptoms resolve after a week or so to be followed by a lingering diarrhea or steatorrhea associated with weight loss.
Table 105-3 Clinical Features of Tropical Malabsorption and Their Causes
| CLINICAL FEATURE(S) | CAUSE(S) | MECHANISM(S) |
|---|---|---|
| Diarrhea | ||
| Pale, bulky stool | Fatty acid and bile malabsorption | |
| Foul-smelling stool | Fat and protein malabsorption | |
| Borborygmi, abdominal fullness | Carbohydrate malabsorption | Bacterial fermentation of unabsorbed carbohydrate |
| Nocturia | Delayed water absorption | Small intestinal disease delays water absorption |
| Pedal edema, skin changes, leukonychia, muscle wasting | Hypoproteinemia and protein-losing enteropathy | |
| Pallor | Anemia due to vitamin B12, folate, iron deficiency | Mucosal disease in duodenum (folate, iron) and ileum (B12) |
| Koilonychia | Iron deficiency | Mucosal disease in duodenum |
| Hyperpigmentation of palms, knuckles, mouth | Vitamin B12 deficiency | Disturbed metabolism of melanin |
| Angular stomatitis, glossitis | Vitamin B deficiency | Mucosal disease of small intestine |
| Night blindness, corneal xerosis, Bitot’s spots | Vitamin A deficiency | Steatorrhea with malabsorption of vitamin A |
| Muscle weakness | Hypophosphatemia, hypokalemia, hypomagnesemia | Mucosal disease with malabsorption or secretion |
| Tetany, carpopedal spasm | Hypocalcemia | Steatorrhea |
| Hemorrhagic diathesis | Vitamin K deficiency | Steatorrhea with malabsorption of vitamin K |
| Lack of taste (ageusia) | Zinc deficiency | Steatorrhea with malabsorption of vitamin D |
| Weight loss | ||
| Ogilvie’s syndrome | Colonic pseudo-obstruction due to electrolyte disorders (e.g., hypokalemia, hypomagnesemia) | Uncoordinated muscle activity and segmentation |
The physical signs that may be found in affected patients (see Table 105-3) (see Chapter 100) include pallor from iron and vitamin B deficiency; angular stomatitis, cheilitis, and glossitis due to vitamin B deficiency; and peripheral edema and skin and hair changes secondary to hypoproteinemia. Hyperpigmentation of the buccal mucosa, palms, and knuckles sometimes is noted (Fig. 105-2) and has been ascribed to vitamin B12 deficiency. Vitamin A deficiency with night blindness, Bitot’s spots, and corneal xerosis and subacute combined degeneration of the spinal cord resulting from vitamin B12 deficiency are much rarer. Fever has been noted in a quarter of patients in South India. Patients are grossly emaciated in the later stages of illness, with muscle weakness, particularly in the proximal muscles.

Peripheral neuropathy may be present, but subacute combined degeneration of the spinal cord, once noted in tropical sprue, is no longer found, perhaps because of earlier diagnosis and treatment. The presence of finger clubbing should suggest other illness such as immunoproliferative small intestinal disease, in which this finding is characteristic (Fig. 105-3
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


