Recent trends and current knowledge on the diagnosis and treatment strategy for gastric mucosa-associated lymphoid tissue (MALT) lymphoma are reviewed. Helicobacter pylori infection plays the causative role in the pathogenesis, and H pylori eradication is the first-line treatment of this disease, which leads to complete remission in 60% to 90% of cases. A Japanese multicenter study confirmed that the long-term outcome of gastric MALT lymphoma after H pylori eradication is excellent. Treatment strategies for patients not responding to H pylori eradication including “watch and wait” strategy, radiotherapy, chemotherapy, rituximab immunotherapy, and combination of these should be tailored in consideration of the disease extent in each patient.
Key points
- •
Infection with H pylori is found in 80% to 90% of gastric MALT lymphoma cases.
- •
First-line treatment of gastric MALT lymphomas should be H pylori eradication independent of the stage.
- •
H pylori eradication achieves complete remission in 60% to 90% of cases.
- •
Strategies for nonresponders to eradication, including “watch and wait,” radiotherapy, chemotherapy, or rituximab immunotherapy, should be tailored.
Introduction
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is an indolent non-Hodgkin lymphoma composed of morphologically heterogeneous small B cells including marginal zone (centrocyte-like) cells, monocytoid cells, and scattered immunoblasts and centroblast-like cells. MALT lymphoma occurs in various extranodal organs, and the stomach is the most common site; it comprises 7% to 9% of all B-cell lymphomas, 3% to 6% of all gastric malignant neoplasms, and 40% to 50% of primary gastric lymphomas. In most patients with gastric MALT lymphoma, Helicobacter pylori plays a causative role in the development of the disease, and the eradication of H pylori leads to a complete remission of the lymphoma in 60% to 90% of cases.
Here we review recent trends and the current knowledge regarding the diagnosis and treatment strategy for patients with gastric MALT lymphoma.
Introduction
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is an indolent non-Hodgkin lymphoma composed of morphologically heterogeneous small B cells including marginal zone (centrocyte-like) cells, monocytoid cells, and scattered immunoblasts and centroblast-like cells. MALT lymphoma occurs in various extranodal organs, and the stomach is the most common site; it comprises 7% to 9% of all B-cell lymphomas, 3% to 6% of all gastric malignant neoplasms, and 40% to 50% of primary gastric lymphomas. In most patients with gastric MALT lymphoma, Helicobacter pylori plays a causative role in the development of the disease, and the eradication of H pylori leads to a complete remission of the lymphoma in 60% to 90% of cases.
Here we review recent trends and the current knowledge regarding the diagnosis and treatment strategy for patients with gastric MALT lymphoma.
Pathogenesis
Helicobacter pylori
In 1991, Wotherspoon and colleagues first reported a link of H pylori with gastric MALT lymphoma by histologic detection of the bacteria in most cases. This association was supported by subsequent epidemiologic and histopathologic studies. Infection with H pylori is observed in 80% to 90% of patients with gastric MALT lymphoma, and 60% to 80% of the cases respond to H pylori eradication therapy. In such H pylori –dependent cases, the growth of lymphoma cells is largely driven by H pylori –generated immune responses including signaling from CD40 and CD86 through bystander T-cell help. A proliferation-inducing ligand (APRIL), a tumor necrosis factor (TNF) superfamily member, produced by macrophages in the H pylori –infected gastric mucosa also plays an important role in promoting the survival and proliferation of neoplastic B cells.
Genetic Aberrations
MALT lymphoma is genetically characterized by the replicable chromosomal translocations t(11;18) (q21;q21)/ API2-MALT1 , t(1;14) (p22;q32)/ BCL10-IGH , t(14;18) (q32;q21)/ IGH-MALT1 , and t(3;14) (p13;q32)/ FOXP1-IGH . These translocations are considered to exert their oncogenic activities through constitutive activation of the nuclear factor kappa B (NF-κB) pathway, leading to expression of several genes for cell survival and proliferation. Among these aberrations, t(11;18)/ API2-MALT1 is the most frequent translocation, which is detected in 15% to 24% of gastric MALT lymphoma cases. The translocation fuses the N-terminal region of the API2 to the C-terminal region of the MALT1 and generates a functional chimeric fusion, which gains the ability to activate the NF-κB pathway. Clinically, t(11;18)/ API2-MALT1 is frequently associated with the absence of H pylori infection, and most the translocation-positive cases do not respond to H pylori eradication therapy. Interestingly, t(11;18)-positive MALT lymphomas rarely transform to diffuse large B-cell lymphoma.
The TNF-α–induced protein 3 gene ( TNFAIP3 , A20 ), which has been recently identified as the target of 6q23 deletion in MALT lymphomas, is an important negative regulator of NF-κB. The mutation and/or deletion of A20 , which leads to A20 inactivation, is observed frequently in MALT lymphoma of the ocular adnexa, salivary glands, thyroid, and liver. Such A20-mediated oncogenic activities in MALT lymphoma are considered to depend on the NF-κB activation triggered by TNF or other unidentified molecules. By contrast, A20 deletion was detected only in 2 of 29 (7%) cases of gastric MALT lymphomas. Further investigations with larger numbers of patients are warranted to determine to what extent A20 inactivation contributes to the development of gastric MALT lymphoma.
Diagnosis
Histopathology
The definite diagnosis of gastric MALT lymphoma should be based on the histopathologic criteria by the World Health Organization classification, using the tissue specimens appropriately obtained by biopsy or surgical resection. Histologically, the small- to medium-sized neoplastic lymphoid cells (centrocyte-like cells) infiltrate around reactive follicles showing marginal zone growth pattern, which often infiltrate into gastric glands causing destruction of the epithelial cells (lymphoepithelial lesions). Immunohistochemically, the tumor cells exhibit CD20 + , CD79a + , CD5 − , CD10 − , CD23 − , CD43 +/− , and cyclin D1 − . When large neoplastic cells are present in solid or sheets, the diagnosis of an associated diffuse large B-cell lymphoma should be made. Staining for Ki-67 may help the identification of diffuse large B-cell lymphoma. The diagnosis should be confirmed by an expert hematopathologist.
The differential diagnosis of gastric MALT lymphoma includes the reactive inflammatory conditions, such as H pylori –related chronic gastritis. Distinction from gastritis is based mainly on the presence of a dense infiltrate of monotonous B cells extending away from lymphoid follicles, the presence of cytologic atypia of lymphoid cells, Dutcher bodies, and characteristic lymphoepithelial lesions. Wotherspoon score is widely used for the confident histologic diagnosis of gastric MALT lymphoma on biopsy specimens ( Table 1 ). The consensus report of the European Gastro-Intestinal Lymphoma Study (EGILS) group recommends that a minimum of 10 biopsy samples should be taken from visible lesions and endoscopically normal-appearing mucosa. The demonstration of immunoglobulin light chain (κ or λ) restriction by immunohistochemistry or in situ hybridization, and analyses for clonality of the rearranged immunoglobulin genes by polymerase chain reaction, may help a diagnosis of B-cell lymphoma. Cytogenetic analyses using G-banding, reverse-transcription polymerase chain reaction, and/or fluorescence in situ hybridization for t(11;18)/ API2-MALT1 or other specific chromosomal translocations are useful for confirming the diagnosis of MALT lymphoma.
| Grade | Description | Histologic Features |
|---|---|---|
| 0 | Normal | Scattered plasma cells in lamina propria; no lymphoid follicles. |
| 1 | Chronic active gastritis | Small clusters of lymphocytes in lamina propria; no lymphoid follicles; no lymphoepithelial lesions. |
| 2 | Chronic active gastritis with florid lymphoid follicle formation | Prominent lymphoid follicles with surrounding mantle zone and plasma cells; no lymphoepithelial lesions. |
| 3 | Suspicious lymphoid infiltrate in lamina propria, probably reactive | Lymphoid follicles surrounded by small lymphocytes that infiltrate diffusely in lamina propria and occasionally into epithelium. |
| 4 | Suspicious lymphoid infiltrate in lamina propria, probably lymphoma | Lymphoid follicles surrounded by centrocyte-like cells that infiltrate diffusely in lamina propria and into epithelium in small groups. |
| 5 | MALT lymphoma | Presence of dense diffuse infiltrate of centrocyte-like cells in lamina propria with prominent lymphoepithelial lesions. |
Endoscopic Findings
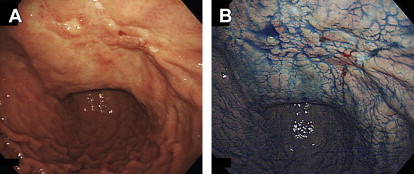
Standard endoscopic or macroscopic classifications for gastric lymphomas have not been established to date. In Western countries, gastric B-cell lymphomas were endoscopically classified either as ulcerative (34%–69%), mass/polypoid (26%–35%), diffusely infiltrating (15%–40%), or other types. In our previous study, 197 consecutive Japanese cases of primary gastric B-cell lymphoma (MALT lymphomas and diffuse large B-cell lymphomas) were macroscopically classified as superficial-spreading (46%), mass-forming (41%), diffuse-infiltrating (6%), or other types (8%). It should be noted that the most frequent macroscopic type in gastric MALT lymphomas is superficial-spreading type ( Fig. 1 ). This type of lymphoma is occasionally misdiagnosed as depressed-type early gastric cancer. By contrast, gastric diffuse large B-cell lymphomas often present as mass-forming type lesions, mimicking advanced gastric cancers. Recently, Zullo and colleagues proposed another endoscopic classification of gastric MALT lymphoma, which includes ulcerative (52%), hypertrophic (24%), normal/hyperemic (13%), exophytic (10%), and petechial hemorrhage types (1%).
Clinical Staging
To determine the optimal management strategy for malignant lymphomas, appropriate clinical staging is essential. It is controversial as to which classification is the best system for staging of gastric MALT lymphoma. Generally, the Lugano International Conference (Blackledge) classification (I, II 1 , II 2 , IIE, or IV; Table 2 ) or Ann Arbor staging system with its modifications by Musschoff and Radaszkiewicz (I 1 E, I 2 E, II 1 E, II 2 E, IIIE, or IV) have been widely applied to patients with gastrointestinal lymphomas. Recently, however, the EGILS consensus report and European Society of Medical Oncology guidelines also recommend to use the Paris staging system, a modification of the TNM system including the degree of the spread of lymphoma assessed by endoscopic ultrasound (see Table 2 ). In addition to esophagogastroduodenoscopy, the following are recommended for the initial staging work-up: physical examination (including peripheral lymph nodes and Waldeyer ring), complete hematologic biochemical examinations (including lactate dehydrogenase and ß 2 -microblobulin), computerized tomography of abdomen and pelvis, and endoscopic ultrasound. We consider that ileocolonoscopy, bone marrow aspiration or biopsy, fluorine-18 fluorodeoxyglucose PET, and endoscopic examinations of the small bowel (balloon-assisted endoscopy or capsule endoscopy) should also be considered.
| Lugano Staging System | Paris Staging System | Tumor Extension | |
|---|---|---|---|
| Stage I | Tumor confined to the GI tract (single primary site or multiple, noncontiguous lesions) | T1m N0 M0 T1sm N0 M0 T2 N0 M0 T3 N0 M0 | Mucosa Submucosa Muscularis propria Serosa |
| Stage II | Tumor extending into abdomen | — | — |
| II 1 | Local nodal involvement | T1-3 N1 M0 | Perigastric lymph nodes |
| II 2 | Distant nodal involvement | T1-3 N2 M0 | More distant regional nodes |
| Stage IIE | Penetration of serosa to involve adjacent organs or tissues | T4 N0-2 M0 | Invasion of adjacent structures with or without abdominal lymph nodes |
| Stage IV | Disseminated extranodal involvement or concomitant supradiaphragmatic nodal involvement | T1-4 N3 M0 T1-4 N0-3 M1 T1-4 N0-3 M2 T1-4 N0-3 M0-2 BX T1-4 N0-3 M0-2 B0 T1-4 N0-3 M2 B1 | Extra-abdominal lymph nodes And/or additional distant GI sites Or non-GI sites Bone marrow not assessed Bone marrow not involved Bone marrow involvement |
Treatments
Helicobacter pylori Eradication
The first-line treatment of all gastric MALT lymphomas is H pylori eradication therapy independent of the stage. In patients with stage I/II 1 disease, complete remission is achieved in 60% to 90% of cases only by H pylori eradication. Histologic evaluation of posttreatment biopsies should be based on the Groupe d’Etude des Lymphomes de l’Adulte grading system ( Table 3 ), because Wotherspoon score (see Table 1 ), recommended for initial diagnosis, is no longer considered adequate for response assessment during follow-up. As for the regimen for H pylori eradication, proton pump inhibitor plus clarithromycin-based triple therapy composed of a double dose of a proton pump inhibitor plus clarithromycin and amoxicillin or metronidazole for 7 or 14 days has been recommended but is now considered obsolete (discussed elsewhere in this issue in the article on practical aspects in choosing an H pylori therapy). Success of bacterial eradication should be confirmed by urea breath test or stool antigen test. A first evaluation of lymphoma regression using endoscopy and biopsy should be performed 3 to 6 months after completion of successful treatment. Further follow-up should be performed every 4 to 6 months thereafter until complete remission (complete histologic response or probable minimal residual disease, see Table 3 ) is documented. Although complete remission is obtained usually within 6 to 12 months, it may be delayed up to 24 to 71 months in some cases.
Related posts:
 Diagnosis of Helicobacter pylori Infection in the Proton Pump Inhibitor Era
Diagnosis of Helicobacter pylori Infection in the Proton Pump Inhibitor Era
 Helicobacter pyloriEradication to Eliminate Gastric Cancer
Helicobacter pyloriEradication to Eliminate Gastric Cancer
 Gastric Cancer Risk in Patients with Helicobacter pylori Infection and Following Its Eradication
Gastric Cancer Risk in Patients with Helicobacter pylori Infection and Following Its Eradication
 Helicobacter pylori
Helicobacter pylori
 When Is Endoscopic Follow-up Appropriate After Helicobacter pyloriEradication Therapy?
Screening to Identify and Eradicate Helicobacter pyloriInfection in Teenagers in Japan
When Is Endoscopic Follow-up Appropriate After Helicobacter pyloriEradication Therapy?
Screening to Identify and Eradicate Helicobacter pyloriInfection in Teenagers in Japan
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


