Chapter 21 The liver in pregnancy
TABLE 21.1 Changes in liver biochemical test levels in normal pregnancy
| Test | Change | Trimester of maximum change |
|---|---|---|
| Albumin | ↓ 10%–60% | Second |
| Gamma globulins | None to slight ↓ | Third |
| Fibrinogen | ↓ 50% | Second |
| Transferrin | ↓ | Third |
| Bilirubin | None | — |
| Alkaline phosphatase | ↓ Two- to fourfold | Third |
| AST | None | — |
| ALT | None | — |
| Cholesterol | ↓ Twofold | Third |
↓, increase; ↓, decrease; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
From Olans LB, Wolf JL. Liver disease in pregnancy. In: Carlson KJ, Eisenstat SA, eds. The Primary Care of Women, 2nd edn. St. Louis: Mosby–Year Book; 2003:531–539.
Overview








Approach to the Pregnant Patient
History










 Headache, peripheral edema, foamy urine, oliguria, and neurologic symptoms may occur in pre-eclampsia
Headache, peripheral edema, foamy urine, oliguria, and neurologic symptoms may occur in pre-eclampsia








TABLE 21.2 Differential diagnosis of elevated serum aminotransferase levels and/or jaundice according to trimester of pregnancy
| Trimester | Differential diagnosis |
|---|---|
| First | Hyperemesis gravidarum |
| Gallstones | |
| Viral hepatitis | |
| Drug-induced hepatitis | |
| Intrahepatic cholestasis of pregnancy∗ | |
| Second | Intrahepatic cholestasis of pregnancy |
| Gallstones | |
| Viral hepatitis | |
| Drug-induced hepatitis | |
| Pre-eclampsia/eclampsia∗ | |
| HELLP syndrome∗ | |
| Third | Intrahepatic cholestasis of pregnancy |
| Pre-eclampsia/eclampsia | |
| HELLP syndrome | |
| Acute fatty liver of pregnancy | |
HELLP, hemolysis, elevated liver tests, low platelets.
From Olans LB, Wolf J. Liver disease in pregnancy. In: Carlson KJ, Eisenstat SA, eds. The Primary Care of Women, 2nd edn. St. Louis: Mosby–Year Book; 2003:531–539.
TABLE 21.3 Rates of recurrence of pregnancy-associated liver disease in subsequent pregnancies
| Disease | Rate of recurrence |
|---|---|
| Intrahepatic cholestasis of pregnancy | 40%–70% |
| HELLP syndrome | 4%–27% |
| Acute fatty liver of pregnancy | 20%–70% in carriers of LCHAD mutation |
| Pre-eclampsia | 2%–43% |
HELLP, hemolysis, elevated liver tests, low platelets; LCHAD, long-chain 3-hydroxyacyl-coenzyme A dehydrogenase.



Diagnostic tests
 The only major restrictions compared with the nongravid state are radiation and gadolinium exposures
The only major restrictions compared with the nongravid state are radiation and gadolinium exposures



 If viral hepatitis is suspected, serologic tests should be checked for the following: hepatitis A (immunoglobulin M [IgM] and IgG antibody to hepatitis A virus [anti-HAV]); hepatitis B (surface antigen [HBsAg] and antibody, core antibody, and, if HBsAg is positive, e antigen and antibody); hepatitis C (antibody to hepatitis C virus [anti-HCV] and possibly HCV RNA). If the patient has traveled to an endemic area, consider testing for hepatitis E (see Chapter 3)
If viral hepatitis is suspected, serologic tests should be checked for the following: hepatitis A (immunoglobulin M [IgM] and IgG antibody to hepatitis A virus [anti-HAV]); hepatitis B (surface antigen [HBsAg] and antibody, core antibody, and, if HBsAg is positive, e antigen and antibody); hepatitis C (antibody to hepatitis C virus [anti-HCV] and possibly HCV RNA). If the patient has traveled to an endemic area, consider testing for hepatitis E (see Chapter 3)




Liver Disorders Unique to Pregnancy
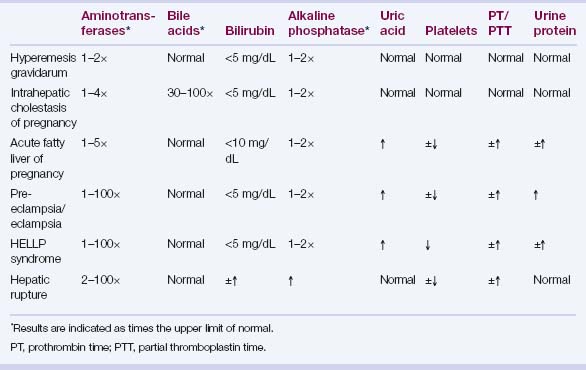
See Table 21.4 for the laboratory findings associated with these disorders.
Hyperemesis gravidarum







Intrahepatic cholestasis of pregnancy



 Gene variants of hepatocanalicular transport proteins (ATP-binding cassette [ABC] transporter B4 = phosphatidylcholine floppase, ABC transporter B11 = bile salt export pump, ABC transporter C2 = conjugated organic anion transporter, ATP8B1 = FIC1) and their regulators (e.g., the bile acid sensor farnesoid X receptor, FXR) found in some patients; incidence of IHCP increased in mothers of children with progressive familial intrahepatic cholestasis (PFIC) type 3
Gene variants of hepatocanalicular transport proteins (ATP-binding cassette [ABC] transporter B4 = phosphatidylcholine floppase, ABC transporter B11 = bile salt export pump, ABC transporter C2 = conjugated organic anion transporter, ATP8B1 = FIC1) and their regulators (e.g., the bile acid sensor farnesoid X receptor, FXR) found in some patients; incidence of IHCP increased in mothers of children with progressive familial intrahepatic cholestasis (PFIC) type 3








