CHAPTER 12 Symptoms of Esophageal Disease
Symptoms related to the esophagus are among the most common in general medical as well as gastroenterologic practice. For example, dysphagia becomes more common with aging and affects up to 15% of persons age 65 or older.1 Heartburn, regurgitation, and other symptoms of gastroesophageal reflux disease (GERD) also are common. A survey of healthy subjects in Olmsted County, Minnesota, found that 20% of persons, regardless of gender or age, experienced heartburn at least weekly.2 Mild symptoms of GERD rarely indicate severe underlying disease but must be addressed, especially if they have occurred for many years. Frequent or persistent dysphagia or odynophagia suggests an esophageal problem that necessitates investigation and treatment. Other less specific symptoms of possible esophageal origin include globus sensation, chest pain, belching, hiccups, rumination, and extraesophageal complaints, such as wheezing, coughing, sore throat, and hoarseness, especially if other causes have been excluded. A major challenge in the evaluation of esophageal symptoms is that the degree of esophageal damage often does not correlate well with the patient’s or physician’s impression of symptom severity. This is a particular problem in older patients, in whom the severity of gastroesophageal reflux–induced injury to the esophageal mucosa is increased despite an overall decrease in the severity of symptoms.3
DYSPHAGIA
PATHOPHYSIOLOGY
The inability to swallow is caused by a problem with the strength or coordination of the muscles required to move material from the mouth to the stomach or by a fixed obstruction somewhere between the mouth and the stomach. Occasional patients may have a combination of the two processes. The oropharyngeal swallowing mechanism and the primary and secondary peristaltic contractions of the esophageal body that follow usually transport solid and liquid boluses from the mouth to the stomach within 10 seconds (see Chapter 42). If these orderly contractions fail to develop or progress, the accumulated bolus of food distends the esophageal lumen and causes the discomfort that is associated with dysphagia. In some patients, particularly older adults, dysphagia is the result of low-amplitude primary or secondary peristaltic activity that is insufficient to clear the esophagus. Other patients have a primary or secondary motility disorder that grossly disturbs the orderly contractions of the esophageal body. Because these motor abnormalities may not be present with every swallow, dysphagia may wax and wane (see Chapter 42).
Mechanical narrowing of the esophageal lumen may interrupt the orderly passage of a food bolus despite adequate peristaltic contractions. Symptoms vary with the degree of luminal obstruction, associated esophagitis, and type of food ingested. Although minimally obstructing lesions cause dysphagia only with large, poorly chewed boluses of foods such as meat and dry bread, lesions that obstruct the esophageal lumen completely lead to symptoms with solids and liquids. GERD may produce dysphagia related to an esophageal stricture, but some patients with GERD clearly have dysphagia in the absence of a demonstrable stricture, and perhaps even without esophagitis.4 Abnormal sensory perception in the esophagus may lead to the perception of dysphagia, even when the bolus has cleared the esophagus. Because some normal subjects experience the sensation of dysphagia when the distal esophagus is distended by a balloon, as well as by other intraluminal stimuli, an aberration in visceral perception could explain dysphagia in patients who have no definable cause.5 This mechanism also may apply to the amplification of symptoms in patients with spastic motility disorders, in whom the frequency of psychiatric disorders is increased.6
DIFFERENTIAL DIAGNOSIS AND APPROACH
Oropharyngeal Dysphagia
Recurrent bouts of pulmonary infection may reflect spillover of food into the trachea because of inadequate laryngeal protection. Hoarseness may result from recurrent laryngeal nerve dysfunction or intrinsic muscular disease, both of which cause ineffective vocal cord movement. Weakness of the soft palate or pharyngeal constrictors causes dysarthria and nasal speech as well as pharyngonasal regurgitation. Swallowing associated with a gurgling noise may be described by patients with Zenker’s diverticulum. Finally, unexplained weight loss may be the only clue to a swallowing disorder; patients avoid eating because of the difficulties encountered. Potential causes of oropharyngeal dysphagia are shown in Table 12-1.
Table 12-1 Causes of Oropharyngeal Dysphagia
| Neuromuscular Causes* |
| Structural Causes |
CNS, central nervous system; UES, upper esophageal sphincter.
* Any disease that affects striated muscle or its innervation may result in dysphagia.
† Many manometric disorders (hypertensive and hypotensive UES, abnormal coordination, and incomplete UES relaxation) have been described, although their true relationship to dysphagia is often unclear.
Esophageal Dysphagia
On the basis of these answers, distinguishing the several causes of esophageal dysphagia (Table 12-2) as a mechanical or a neuromuscular defect and postulating the specific cause are often possible (Fig. 12-1).
Table 12-2 Common Causes of Esophageal Dysphagia
| Motility (Neuromuscular) Disorders |
| Primary Disorders |
| Secondary Disorders |
| Structural (Mechanical) Disorders |
| Intrinsic |
| Extrinsic |
LES, lower esophageal sphincter.
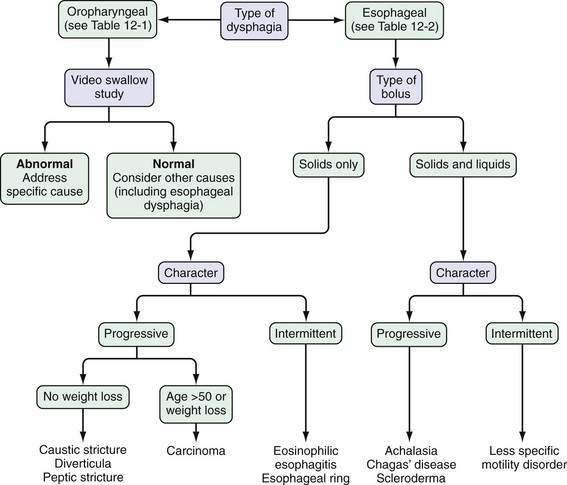
Patients who report dysphagia with solids and liquids are more likely to have an esophageal motility disorder than mechanical obstruction. Achalasia is the prototypical esophageal motility disorder in which, in addition to dysphagia, many patients complain of bland regurgitation of undigested food, especially at night, and of weight loss. By contrast, patients with spastic motility disorders such as diffuse esophageal spasm may complain of chest pain and sensitivity to hot or cold liquids. Patients with scleroderma of the esophagus usually have Raynaud’s phenomenon and severe heartburn. In these patients, mild complaints of dysphagia can be caused by a motility disturbance or esophageal inflammation, but severe dysphagia almost always signals the presence of a peptic stricture (see Chapters 35 and 43).
In patients who report dysphagia only after swallowing solid foods and never with liquids alone, a mechanical obstruction is suspected. A luminal obstruction of sufficiently high grade, however, may be associated with dysphagia for solids and liquids. If food impaction develops, the patient frequently must regurgitate for relief. If a patient continues to drink liquid after the bolus impaction, large amounts of that liquid may be regurgitated. In addition, hypersalivation is common during an episode of dysphagia, thereby providing even more liquid to regurgitate. Episodic and nonprogressive dysphagia without weight loss is characteristic of an esophageal web or a distal esophageal (Schatzki) ring. The first episode typically occurs during a hurried meal, often with alcohol. The patient notes that the bolus of food sticks in the lower esophagus; it often can be passed by drinking large quantities of liquids. Many patients finish the meal without difficulty after the obstruction is relieved. The offending food frequently is a piece of bread or steak—hence the term steakhouse syndrome.7 Initially, an episode may not recur for weeks or months, but subsequent episodes may occur frequently. Daily dysphagia, however, is likely not caused by a lower esophageal ring (see Chapter 41).
If solid food dysphagia is clearly progressive, the differential diagnosis includes peptic esophageal stricture and carcinoma. Benign esophageal strictures develop in some patients with GERD. Most of these patients have a long history of associated heartburn. Weight loss seldom occurs in patients with a benign lesion, because these patients have a good appetite and convert their diet to high-calorie soft and liquid foods to maintain weight (see Chapter 43). Patients with carcinoma differ from those with peptic stricture in several ways. As a group, the patients with carcinoma are older and present with a history of rapidly progressive dysphagia. They may or may not have a history of heartburn, and heartburn may have occurred in the past but not the present. Most have anorexia and weight loss (see Chapter 46). True dysphagia may be seen in patients with pill, caustic, or viral esophagitis; however, the predominant complaint of patients with these acute esophageal injuries is usually odynophagia. Patients may present with food bolus impaction, and eosinophilic esophagitis should be considered in the differential diagnosis of all patients (particularly those who are young) who present with dysphagia (see Chapter 27).8
After a focused history of the patient’s symptoms is obtained, a barium radiograph, including a solid bolus challenge, is often advocated as the first test. Alternatively, many experts have advocated endoscopy as the first test, especially in patients with intermittent dysphagia for solid food suggestive of a lower esophageal ring or with pronounced reflux symptoms. The choice of the initial test should be based on local expertise and the preference of the individual health care provider. If the barium examination demonstrates an obstructive lesion, endoscopy is usually done for confirmation and biopsy. Endoscopy also permits dilation of strictures, rings, and neoplasms. Empirical dilation of the esophagus is often performed in patients with a suggestive history and normal endoscopic examination,9 but the safety and efficacy of this approach have been questioned.10 If the barium examination is normal, esophageal manometry is often performed to look for a motility disorder. Some patients with reflux symptoms and dysphagia, a normal barium study or endoscopy, or both, will respond to a trial of gastric acid suppressive therapy.
ODYNOPHAGIA
Like dysphagia, odynophagia, or painful swallowing, is specific for esophageal involvement. Odynophagia may range from a dull retrosternal ache on swallowing to a stabbing pain with radiation to the back so severe that the patient cannot eat or even swallow his or her own saliva. Odynophagia usually reflects an inflammatory process that involves the esophageal mucosa or, in rare instances, the esophageal muscle. The most common causes of odynophagia include caustic ingestion, pill-induced esophagitis, radiation injury, and infectious esophagitis (Candida, herpesvirus, and cytomegalovirus; Table 12-3). In these diseases, dysphagia also may be present, but pain is the dominant complaint. Odynophagia is an infrequent complaint of patients with GERD and, when present, usually is associated with severe ulcerative esophagitis. In rare cases, a nonobstructive esophageal carcinoma can produce odynophagia. Because many of the diseases that cause odynophagia have associated symptoms and signs, a carefully taken history can often lead directly to a diagnosis. For example, a teenager who takes tetracycline for acne and in whom odynophagia develops most likely has pill dysphagia, an immunocompromised patient with odynophagia is likely to have an infectious cause, and a patient with GERD is likely to have severe peptic esophagitis. On the other hand, gastrointestinal endoscopy to visualize and obtain biopsies of the esophageal mucosa is required to confirm a specific diagnosis in most patients with odynophagia.
Table 12-3 Causes of Odynophagia
| Caustic Ingestion |
| Pill-Induced Injury |
| Aspirin and other NSAIDs |
| Infectious Esophagitis |
| Viral |
| Bacterial |
| Mycobacteria (tuberculosis or Mycobacterium avium complex) |
| Fungal |
| Candida albicans |
| Histoplasmosis |
| Protozoan |
| Cryptosporidium |
| Pneumocystis |
| Severe Reflux Esophagitis |
| Esophageal Carcinoma |
NSAIDs, nonsteroidal anti-inflammatory drugs.
GLOBUS SENSATION
Globus sensation is a feeling of a lump or tightness in the throat, unrelated to swallowing. Up to 46% of the general population experience globus sensation at one time or another.11 The sensation can be described as a lump, tightness, choking, or strangling feeling, as if something is caught in the throat. Globus sensation is present between meals, and swallowing of solids or large liquid boluses may give temporary relief. Frequent dry swallowing and emotional stress may worsen this symptom. Globus sensation should not be diagnosed in the presence of dysphagia or odynophagia.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


