Robotic Resection
Leela M. Prasad
Sonia L. Ramamoorthy
The introduction of laparoscopy to colorectal surgery has created a paradigm shift in the approach to colectomy both for malignant and benign disease. The advantages of minimally invasive surgery over the traditional open approach are clearly evident when short- and long-term patient outcomes are compared. Trials designed to show oncological equivalence have demonstrated that there is no disadvantage in using laparoscopy for cancer patients (1).
Robot-assisted surgery is being increasingly utilized in a number of surgical specialties. Early reports in the United States have demonstrated the safety and feasibility of robot-assisted colectomy using the da Vinci system (2,3). Over the course of the past 5 years, robotic colorectal surgery has increased in popularity, particularly for pelvic procedures. However, the advantage of robotic assistance in a standard colectomy is still unclear (4). In this chapter, the surgical technique pros and cons and outcomes of robot-assisted right hemicolectomy will be discussed.
Advantages of the Robotic Approach
The potential advantages of robotic surgery include improved visualization, tremor filtration, motion scaling, and seven degrees of freedom provided by the robot’s unique endowristed instruments. Surgeon comfort is facilitated by the ergonomically designed console and the robotic camera that is surgeon controlled can be zoomed-in to provide high magnification. With the many advantages of the system, technically challenging tasks such as intracorporeal suturing and vessel ligation are made easier. A hand-sewn intracorporeal anastomosis that is extremely challenging when laparoscopically performed is now possible with the robot.
The high definition, 3D imaging of the robotic system improves visualization and surgeon accuracy. Whether this ever translates into improved oncological outcomes with high vascular pedicle ligation, improved node retrieval, and negative radial margins remains to be seen. An important advantage unique to the robotic
system is the ability of the surgeon to control three individual instrument arms. This enables the third arm to be placed in a position of fixed and stable retraction while the other two arms are used for precise retraction and dissection at the plane of dissection.
system is the ability of the surgeon to control three individual instrument arms. This enables the third arm to be placed in a position of fixed and stable retraction while the other two arms are used for precise retraction and dissection at the plane of dissection.
Drawbacks of the Robotic Approach
Haptic Feedback
In the transition from open to laparoscopic surgery, tactile sense was compromised. However, with experience and better instrumentation these challenges are gradually being overcome. Robotic surgery offers even less haptic feedback and therefore the surgeon must “learn” appropriate grasping pressures so as to avoid damage to the bowel and other structures. Much of that feedback relies on the lines of tissue tension upon which the extent of retraction and force applied on the tissues must be based. The three-dimensional imaging does go a long way in recognizing these visual cues (5). Initially developed as a platform for cardiac surgery, the robotic system is limited in the range of available instruments for surgery on the bowel. New instruments for the robotic arms are slowly evolving as the utilization of robotic assistance increases across different surgical specialties. Figure 5.1 depicts the tissue graspers currently available for colorectal surgery.
Cost
There is much debate over the costs of robot-assisted surgery. In a study by Delaney et al. (3), a direct comparison of robot-assisted with laparoscopic colectomy was performed using case matched controls. The authors concluded that although a robot-assisted colectomy was safe and feasible, the additional cost was a matter of concern. A similar study by Rawlings et al. (6) confirmed the safety and efficacy of robotic colectomy but reported similar findings of a longer operative time and a higher cost. We recently conducted a cost analysis in a series of 40 consecutive robotic right hemicolectomies and compared it to the cost associated with a laparoscopic right colon resection (7). The initial investment to procure the robot as well as the maintenance and ongoing costs for the robot was also considered. Costs associated with a robotic procedure were higher in every cost category.
 Figure 5.1 Bowel graspers for the da Vinci robot. |
Setup and Preparation
The entire robotic system is a bulky apparatus consisting of the robotic cart, the vision cart, and the surgeon’s console, which can take up a significant amount of space in the operating room (OR). Selecting an OR of sufficient size and establishing dedicated ORs for robotic surgery limit frequent transportation of the entire apparatus from one room to another. The robot, the anesthesia trolley, the mayo stand, and the operating table should be positioned before the patient is brought into the OR. As the robotic cart is used in different positions for different procedures, the setup of the OR may differ for each procedure. Figure 5.2 demonstrates a possible OR setup for a right hemicolectomy.
On average, each robotic instrument can be used up to ten times, but this can vary with the type of instrument used. The validity of the required robotic instruments must be verified before the procedure to limit intraoperative delays. Draping the robotic arms with the specially crafted disposable drapes and calibration of the robotic camera are other aspects of robot setup that must be performed by the scrub
nurse. Significant time can be saved by using an OR nursing team trained in the setup and functioning of the robot.
nurse. Significant time can be saved by using an OR nursing team trained in the setup and functioning of the robot.
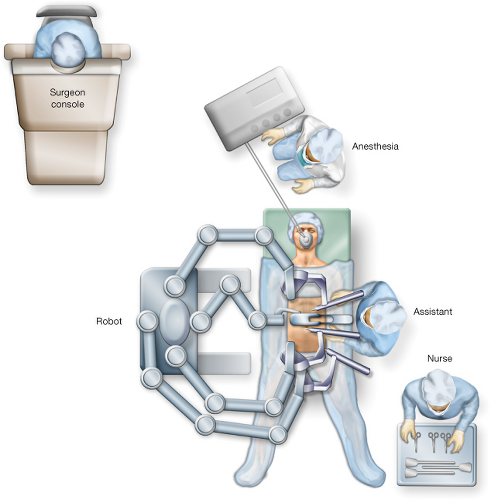 Figure 5.2 Operating room setup for robotic right hemicolectomy. |
Patient Positioning
For a right hemicolectomy, either a supine or lithotomy position can be used. Lithotomy allows for some excursion of the robot arms between the legs if needed, although this must be weighed against the interference from the stirrups that are used for lithotomy positioning. Since access to the perineum is not necessary for right colectomy, the split-leg stirrups are optimal when a lithotomy position is chosen. Both arms are tucked in beside the patient and the patient is secured to the operating table using a suction operated bean bag. Careful attention should be paid to protecting pressure points with adequate padding to avoid postoperative neuropathy. Additional shoulder harnesses are placed to support the patient when placed in the Trendelenburg position. Patient positioning is tested for security before the operative site is prepped and draped to enable changes to be made if required.
The robot is brought in from the right side, and the bedside assistant and scrub nurse are on the patient’s left. Once the robot is docked, the patient position cannot be altered without undocking the robot.
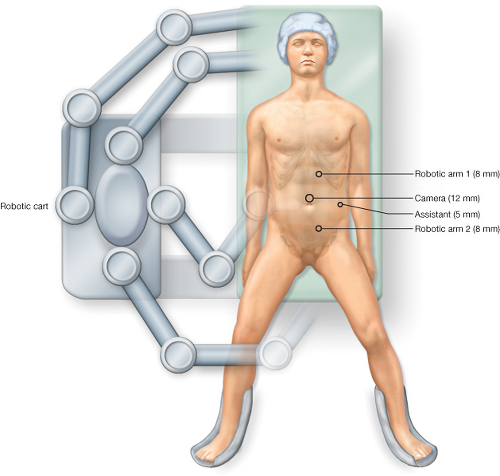 Figure 5.3 Robotic port placement (three robotic ports). |
 Figure 5.4 Robotic port placement (four robotic ports). |
Port Placement
Port placement is vital for any robotic procedure as slight errors in port position can cause external arm collisions that can significantly reduce the intraabdominal range of movement of the robotic instruments. We routinely use just two of the three robotic instrument arms for the procedure and the port configuration is as depicted in Figure 5.3. Alternatively, the procedure can be performed using all four robotic arms as shown in Figure 5.4




Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
