Robotic Left Colon and Rectal Resection
Leela M. Prasad
Slawomir Marecik
Since the first laparoscopic cholecystectomy in the United States in 1988, the evolution of surgical technique has seen a minimally invasive revolution! Laparoscopic surgery is now accepted as a standard of care for colonic resections and is being increasingly offered to patients requiring a rectal resection. Despite its widespread use, laparoscopic surgery poses significant technical challenges to the colorectal surgeon. This is probably why the majority of colorectal procedures in the United States are still being performed through the traditional open approach.
The technical advantages of the Da Vinci® Robotic system (Intuitive Surgical, Sunnyvale, CA, USA) with true three-dimensional imaging, tremor filtration, a stable camera platform, and endowristed movements have attempted to overcome the technical limitations of current laparoscopic instrumentation. These advantages have the potential to benefit patients in terms of possible better oncological and functional outcomes. The surgeon also stands to benefit from the improved ergonomics of the robot that can now avoid the abnormal posturing and hand configuration associated with laparoscopic surgery.
Right at the outset, it should be mentioned that robotics in surgery is a new technology, and the experience with its use in colorectal surgery is probably less, as compared to its use in other surgical fields. At the same time different groups working independently have confirmed the safety and feasibility of robotic assistance in a number of colorectal procedures. At present, there exist a number of colorectal applications of the robot, each with its unique cart position and port placement. This presents a number of options to the colorectal surgeon to suit various patient populations and tumor locations. The purpose of this chapter is to present under one head the various options for robotic assistance in left colon and rectal resections.
It is presumed that the reader is familiar with the parts and setup of the Da Vinci robot, and is proficient with its basic positioning and functioning. This chapter focuses on elaborating the specific cart positions, port placements, and surgical steps essential for robot-assisted left colon resections. As there is no substitute for mentored surgical training, a study of the surgical techniques presented here probably requires initial mentoring for the colorectal surgeon new to robotic technology.
In an attempt to present systematically to the reader the different surgical techniques, the left colon and rectum have been addressed in different chapters. Quite often, resection of the left colon involves mobilization of the upper rectum and a rectal resection always requires mobilization of the left colon to some extent. To maintain some degree of continuity and to enable a comprehensive presentation of the principles of robotic colorectal surgery, some details of robotic rectal dissection have been included here as well.
Finally, it should be appreciated that robotic technology as a whole is rapidly evolving. The Da Vinci Robot itself is in its second version with longer and more maneuverable arms, better ergonomics, and high definition imaging. It is possible that as robotic technology evolves, the techniques presented here might give way to new and better applications of the robot. The need for more precise and ergonomic surgical instruments constantly drives technology to develop better and more efficient tools. It is important to always keep in perspective the primary goal, that is, a better and safer patient care, when evaluating and using these new technologies.
Robot-Assisted Surgical Options
A significant limitation of the robotic system is its restricted surgical field for a given cart position. This enables a precise dissection in one quadrant of the abdomen while limiting access to another without shifting the robotic cart. Every change in robotic cart position requires a complete undocking of the robot, moving the cart to a new position and redocking the robot in the required position. This significantly adds to the operating time.
A colon or rectal resection involves a precise dissection of the tumor/diseased area and a sufficient mobilization of the remaining colon to achieve a tension-free anastomosis. This therefore expands the working surgical field to include a number of abdominal quadrants. As the Da Vinci Robot has a limited access with one cart position, a number of different options have been proposed for the optimal use of the robot in a left colon/rectal resection. Options vary from using the robot in one position to shifting the robotic cart three times during a single procedure. To limit the number of changes in cart position, attempts have to be made to restrict the use of the robot for a part of the procedure or to tailor the use of the robot according to the patient’s habitus, tumor location or colonic anatomy. All the feasible options of robot-assisted left colon/rectal resection have been presented in this chapter. The final choice on the extent of robotic assistance and the number of cart positions should ideally be made on an individual basis.
The Laparoscopic–Robotic “Hybrid Procedure”
The maximal advantage of the robotic system is probably best appreciated in the rectal dissection. The deep retraction along with the precise dissection required to achieve an intact mesorectal envelope while preserving the autonomic nerves is probably what makes a laparoscopic rectal excision for cancer particularly challenging. This technical challenge is more appreciated in the obese, male pelvis, when resecting the mid or low rectal lesion. It is here that the advanced dexterity of the robotic system probably has the potential to offer the greatest benefit.
A rectal resection for cancer requires a total mesorectal excision along with the mobilization of the descending colon, with or without the splenic flexure in order to achieve a tension-free anastomosis. Unlike laparoscopic rectal dissection, laparoscopic mobilization of the descending colon is fairly easily accomplished. The robot could also be effectively used for this mobilization but would probably require a change in cart position. This change in cart position would be more likely when resecting a low rectal tumor, when operating in an obese individual or with a high-riding splenic flexure. These situations would probably expand the surgical field out of the range of the robotic instruments if the position of the robot is not changed.
Taking the “best from both worlds” as it were, a hybrid technique using laparoscopy for the left colon mobilization and the robot for the rectal dissection has been suggested.
This maximizes the advantage of the robot where it is most beneficial, that is, the rectal dissection and overcomes its limitation of a restricted access by using laparoscopic technique for the descending colon mobilization.
This maximizes the advantage of the robot where it is most beneficial, that is, the rectal dissection and overcomes its limitation of a restricted access by using laparoscopic technique for the descending colon mobilization.
The extent of colonic mobilization is largely determined by the level of the lesion and the redundancy of the sigmoid colon. The need for splenic flexure mobilization is often appreciated once the descending colon is completely mobilized. Using laparoscopy for the left colon mobilization provides the flexibility to mobilize a length of colon required to achieve a tension-free anastomosis, which is the main objective. Using the robot for the entire procedure would most likely require more than one cart position if a high-riding splenic flexure and a low rectal lesion have to be addressed during the same procedure. Eliminating the increased time for changing robotic cart positions is an advantage of the hybrid procedure.
Options for Robot-Assisted Left Colon/Rectal Dissection
The following options have been described:
Robotic left colon/sigmoid resection
Robotic low anterior resection’single cart position
Robotic low anterior resection’multiple cart positions
Hybrid procedure (laparoscopic left colon mobilization + robotic rectal dissection)
Robotic abdominoperineal resection (APR)
Principles of Robotic Cart Positioning
The robotic cart is always placed on the side of dissection. This enables the robotic arms that arch away from the robotic cart to be directed back toward the site of dissection. Based on this principle, for dissection of the left colon the cart is placed on the left side of the patient, and for a rectal dissection the best position for the robotic cart would be between the patient’s legs. As an anterior resection always requires some mobilization of the left colon in addition to the rectal mobilization, a totally robotic anterior resection would theoretically require two cart positions, that is, the position between the legs for the rectal dissection and the robotic cart placed by the patient’s left side for the left colon mobilization.
Changing cart positions during the procedure adds significantly to operating time. This is why a position by the patient’s left hip has been described to address the rectum as well as the left colon with the robot in one cart position. The left hip position though not ideal for either a rectal dissection or for a left colon mobilization, is an effective compromise and works in a number of patients. However, in patients with a low rectal lesion, or with a high-riding splenic flexure, the left hip position may not provide the required range of movement to the robotic arms. In such cases, shifting the robotic cart between the legs for the rectal dissection and to the left side or even besides the patient’s left arm for the splenic flexure is required.
To summarize, there are three robotic cart positions described for the left colon and rectum. Table 11.1 lists these positions with the surgical access provided in each position. Figures 11.1–11.3 graphically depict these positions.
The efficacy of different robotic cart positions also varies with the body habitus of the patient. In a short, thin patient of low body mass index (BMI), the position by the left hip alone might provide adequate access to the pelvic floor as well as the splenic flexure. In a tall patient with a high BMI, this might not be the case and a change in cart position may be required for a totally robotic procedure.
The close proximity of the left hip and left arm positions for the robotic cart makes it easier to sometimes move the patient about the stationary robotic cart instead of moving the cart about the patient. If the rectum, sigmoid, and descending colon
are mobilized with the robot in the left hip position, but the robotic arms do not reach the splenic flexure, the robot can be undocked and the patient rotated around the stationary robotic cart so that the robot is now by the patient’s left arm. The splenic flexure can be easily mobilized in this position to complete the colon mobilization. This maneuver may save operative time.
are mobilized with the robot in the left hip position, but the robotic arms do not reach the splenic flexure, the robot can be undocked and the patient rotated around the stationary robotic cart so that the robot is now by the patient’s left arm. The splenic flexure can be easily mobilized in this position to complete the colon mobilization. This maneuver may save operative time.
Table 11.1 Available Robotic Cart Positions | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
It is important to begin every robot-assisted procedure with a preplanned cart position or a plan to use multiple cart positions. A knowledge of the different cart positions and the surgical access offered by each position is essential in this planning. Careful consideration should be given to the patient’s height, BMI, and tumor location. The first step in the preoperative planning of cart positions is to decide whether it is possible to complete the entire procedure in a particular patient with a single position of the robotic cart (Fig. 11.4). This is more likely to be possible in a short, thin patient with a high rectal lesion. As we move to the other end of the spectrum to a tall, obese patient with a low rectal lesion, it is more likely that a change in cart position will be required to complete the procedure robotically. One then has to decide whether to opt for a totally robotic procedure with a change in cart position, or to use the hybrid procedure, reserving the robot for the rectal dissection alone.
As the greatest advantage of the robot is probably for rectal dissection, some centers have adopted the hybrid procedure for all anterior resections irrespective of patient factors. In this procedure, the robot is used for the rectal dissection alone from a position between the patient’s legs. This position is the most ideal for rectal mobilization. While the algorithm is clear at the two ends of the spectrum, there is insufficient data at this stage to make any recommendation for patients in between. For this group of patients, any of the three options of a totally robotic procedure with a single cart position, a totally robotic procedure with multiple cart positions, or a hybrid procedure are acceptable.
Due to lack of data at this stage, it is premature to make any evidence-based recommendation on the ideal use of the robot in left colon/rectal resections. However, it has been our experience that the robot offers the greatest benefit for rectal dissection, which is best achieved with the robot placed between the patient’s legs. At the time of writing this chapter, we use the hybrid procedure for all low anterior resections.
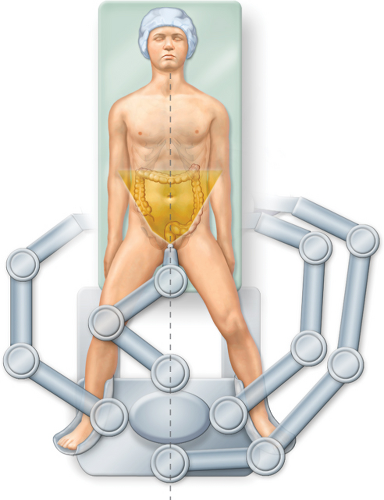 Figure 11.1 Robotic cart between the legs. |
Patient Positioning
The patient is placed on the operating table in a modified lithotomy position with the legs in Allen stirrups and minimal flexure of the hips. The patient’s arms are placed at the side. We use a suction operated bean bag underneath the patient, which is brought up on either side to cradle the patient and support both upper limbs. It is important to place adequate padding between the bean bag and the patient so that there is no contact between the two. We use gel pads beneath the patient and on either side of each arm. Additional foam padding is provided over each shoulder. Care should be taken to ensure that all pressure points and bony prominences are adequately padded and protected.
The bean bag together with the patient is fixed to the operating table with the help of adhesive strapping over the patient’s chest. Shoulder supports, fixed to the operating table, are placed against the bean bag, above the shoulders. These support the patient
when placed in steep Trendelenburg position. This method of immobilization and padding is routine for any minimally invasive resection of the left colon/rectum and is not specific for robotic surgery. However, it should be noted that as the majority of the procedure for a left colon resection is performed with the patient in Trendelenburg position with a left upward tilt, the right side of the patient needs careful attention while padding the pressure points. We routinely use a three-way rectal irrigation tube for a distal rectal washout prior to rectal transection. This is placed at the time of initial positioning.
when placed in steep Trendelenburg position. This method of immobilization and padding is routine for any minimally invasive resection of the left colon/rectum and is not specific for robotic surgery. However, it should be noted that as the majority of the procedure for a left colon resection is performed with the patient in Trendelenburg position with a left upward tilt, the right side of the patient needs careful attention while padding the pressure points. We routinely use a three-way rectal irrigation tube for a distal rectal washout prior to rectal transection. This is placed at the time of initial positioning.
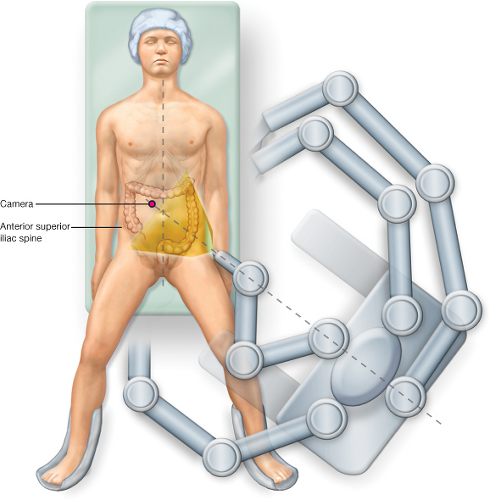 Figure 11.2 Robotic cart in left hip position. |
Operating Room Setup
The operating team consists of the surgeon at the console, a bedside assistant, a scrub nurse, and a circulator. It is necessary for the bedside assistant to have experience with laparoscopic surgery and robotic instrumentation. It is also beneficial for the nursing staff to be familiar with the robotic instruments, setup, and draping. This facilitates a harmonious cooperation between the entire surgical team.
The operating room setup should take into consideration the changes in robotic cart position expected during the procedure. A setup designed to provide the required space around the robotic cart will significantly increase the efficiency in the change in cart position. From Figure 11.5A it can be appreciated that the robotic cart can be moved to
all three described positions without changing the position of the scrub nurse. If, however, a single cart position between the patient’s legs is used, the operating room setup can be accordingly modified (Fig. 11.5B). Two additional points need to be considered here. First, as the assistant stands on the patient’s right, there should be at least one monitor available on the patient’s left side, preferably over the patient’s left shoulder. Second, one of the major roles of the bedside assistant is to clean the robotic laparoscope and replace the scope with another lens, that is, 0 or 30 degree. It is very convenient to have the fluid warmer with the robotic laparoscopes at the left of the bedside assistant. This makes the cleaning and replacement of the lens very quick and efficient.
all three described positions without changing the position of the scrub nurse. If, however, a single cart position between the patient’s legs is used, the operating room setup can be accordingly modified (Fig. 11.5B). Two additional points need to be considered here. First, as the assistant stands on the patient’s right, there should be at least one monitor available on the patient’s left side, preferably over the patient’s left shoulder. Second, one of the major roles of the bedside assistant is to clean the robotic laparoscope and replace the scope with another lens, that is, 0 or 30 degree. It is very convenient to have the fluid warmer with the robotic laparoscopes at the left of the bedside assistant. This makes the cleaning and replacement of the lens very quick and efficient.
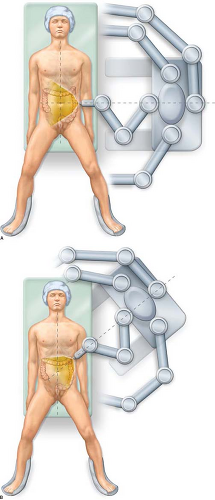 Figure 11.3 A. Robotic cart in left flank position. B. Robotic cart in left arm position. |
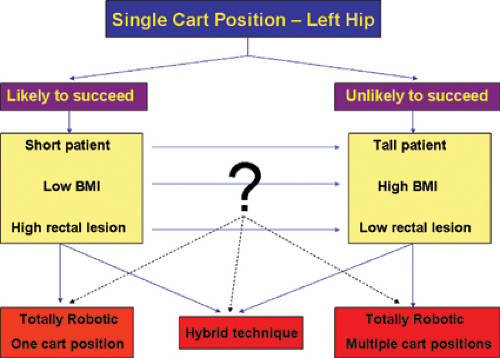 Figure 11.4 Preoperative planning of cart position. |
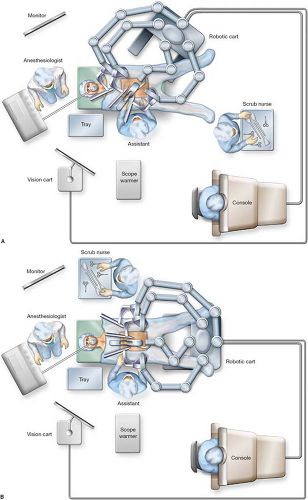 Figure 11.5 A. Room setup for cart in left side position. B. Room setup for cart in between the legs. |
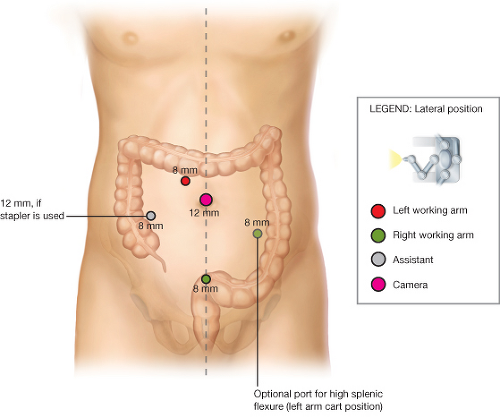 Figure 11.6 Port placement for left colon/sigmoid resection. |
Instruments
Robotic Instruments
Camera 0 and 30 degree
Robotic hook cautery or hot shears
Fenestrated bipolar grasper or Maryland bipolar forceps
Cadiére forceps
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


