Chapter 11 Postsurgical Endoscopic Anatomy
 Video related to this chapter’s topics: Post-Operative Endoscopic Anatomy
Video related to this chapter’s topics: Post-Operative Endoscopic Anatomy
Introduction
Patients who have undergone surgical procedures that alter the anatomy of the upper gastrointestinal (GI) tract are often referred for endoscopic evaluation.1 If meaningful and accurate diagnostic information is to be obtained in these patients, it is important that the endoscopist fully understand the anatomic changes resulting from the surgical procedures.2 Knowledge of the new anatomy is essential to define the type of endoscope and accessories and to determine the need for supplementary studies during or before the endoscopic procedure.3,4 In addition, accurate interpretation of endoscopic findings may permit the endoscopist to identify an unknown previous surgical procedure. This chapter discusses the most common operations in the upper GI tract that are relevant to the endoscopist. Technical details and common variations are described for each surgical procedure and correlated to the findings and to the anatomic alterations observed endoscopically. Surgical terms are also presented to assist the endoscopist in the interpretation of the surgical reports, which should always be reviewed before the endoscopic examination.
Antireflux Procedures
Nissen Fundoplication
Fundoplications to treat gastroesophageal reflux disease (GERD) are performed without gut resection to restore the competency of the cardia (Fig. 11.1). The plication has to be created over the distal esophagus just proximal to the cardioesophageal junction to be effective.5 Modifications to the original fundoplication described by Nissen decreased the incidence of postoperative gas-bloat syndrome and dysphagia at the same time that the laparoscopic approach proved to be safe and reliable.6–10 Shortening from 5 cm to 2 cm and loosening of the fundoplication resulted in the so-called floppy Nissen, which was performed laparoscopically and became the surgical “gold standard” treatment for GERD.11
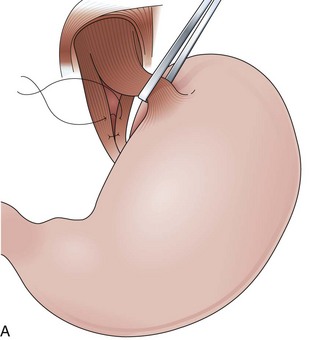
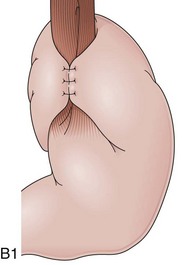
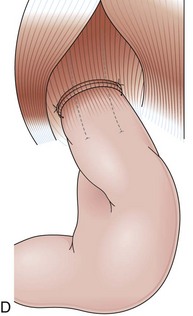

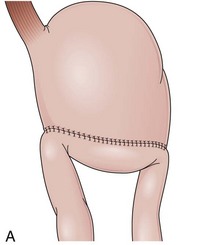
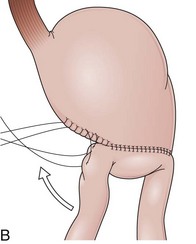
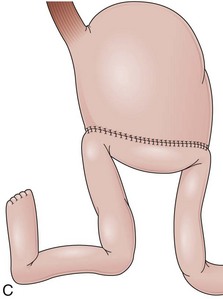
The distal esophagus, the cardioesophageal junction, the gastric fundus, and the right and left crura are dissected in the same way for the open or laparoscopic procedure. Careful dissection is required to avoid transection of the nerve of Latarjet on the right side of the stomach. After reduction of the hernia, the left and right crura are approximated by sutures, gently snuggling the hiatus around the esophagus, which accommodates a previously inserted 60-Fr dilator (Fig. 11.1A). Division of the short gastric vessels may be required to mobilize the fundus.12,13 The gastric fundus is passed behind the esophagus from left to right creating a 360-degree wrap by the placement of two or three sutures involving stomach-esophagus-stomach in the anterior portion of the wrap. The anterior and posterior vagus nervus are usually contained into the wrap, attached to the esophagus. At the end of the procedure, the wrap must lie below the diaphragm without tension (Fig. 11.1B-1).14,15
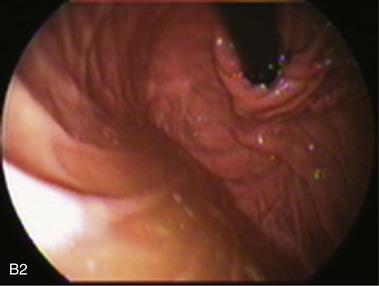
An intact Nissen fundoplication appears to the endoscopist as a narrow, easily transposable distal esophagus, with noninflamed mucosa and reduced distention to air insufflation. An encircling redundant fold overlies the cardia on a retroflexed view and snuggles the endoscope. Edema accentuates the prominent cardia in the early postoperative setting, and the area of the fundus becomes less capacious than normal. Late evaluation of the wrap may reveal several rugal folds parallel to each other and to the markings on the insertion tube of the endoscope (Fig. 11.1B-2). Although this is a 360-degreee wrap, endoscopically the redundant fold appears as a 270-degree free cuff margin because the border continuous with the lesser curvature is not evident.16 The crural closure should maintain the cardia below the diaphragm with the stomach completely insufflated with air. Occasionally, sutures in the distal esophagus may be observed, indicating migration through the wall or inappropriate penetration depth of the stitches during the procedure; this may or may not be associated with symptoms.17
Findings that could be associated with failure of the fundoplication include esophagitis, lack of the encircling fold on a retroflexed view, patulous gap between the endoscope tube and the wrap, migration of the wrap through an enlarged esophageal hiatus, hourglass appearance of the proximal stomach indicating slippage through the valve, and irregularity in the dome shape of the fundus indicating parahiatal hernia. The squamocolumnar junction located more than 1 cm proximal to the margin of the wrap has been reported to be a major endoscopic clue in diagnosis of postfundoplication problems.18 Gastric food retention may be related to damage to the vagus nerves during the procedure.19 Some patients with persistent dysphagia have a tight wrap that causes resistance to the advance of the endoscope, and these patients may benefit from endoscopic dilation.20
Partial Fundoplications (Dor and Toupet)
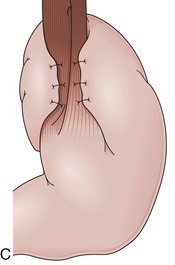
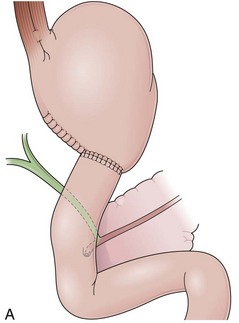
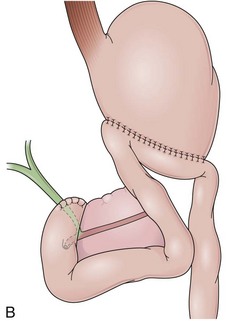
Partial fundoplications are created with the fundus involving partially the distal esophagus. A Dor fundoplication is performed anteriorly, and a Toupet fundoplication is performed posteriorly (Fig. 11.1C and D). Both procedures can be performed to treat GERD; however, they are best indicated in patients who underwent a Heller myotomy (Dor) or with impaired esophageal body motility (Toupet).21–23 Partial fundoplications also have a prominent fold overlying the cardia, which is not less evident than 360-degree wraps when observed endoscopically.24
Belsey Mark IV
With the advent of laparoscopy, the Belsey Mark IV fundoplication is performed only occasionally because it requires a thoracotomy. A circumferential invagination of the distal esophagus into the proximal stomach is performed with two layers of stitches, including anchoring to the diaphragma in the last one. The crura are also sutured to narrow the esophageal hiatus. The final result is a 270-degree wrap around the distal esophagus, placed in the abdomen, and a hiatal repair (Fig. 11.1E). Endoscopically, Belsey Mark IV and Nissen fundoplications are similar, with folds encircling the endoscope at the level of the cardia. However, coils of gastric rugae as seen after Nissen repair are not evident, and there is an anterior compression that corresponds to the attachment of the esophagus to the diaphragm.16
Collis Gastroplasty
A short esophagus, usually caused by chronic scarring resulting from GERD, can be repaired surgically through a Collis gastroplasty. This gastroplasty creates a tubular segment of stomach in continuity to the esophagus, long enough to be encircled by a 360-degree fundoplication placed below the diaphragm. The fundoplication around this tubular segment within the positive pressure of the abdomen prevents the gastroesophageal reflux.25 Short esophagus is declining possibly because patients with GERD are medically diagnosed and treated earlier.26 Endoscopically, the squamocolumnar junction is observed above a short tubular segment of stomach, which may not distend properly because of the wrap. The Collis gastroplasty resembles the Nissen fundoplication on a retroflexed view with a less capacious fundus.
Operations without Alteration of the Pancreaticobiliary Anatomy
Billroth I
Billroth I is a type of reconstruction after a partial gastrectomy in which the stomach is anastomosed to the duodenum (Fig. 11.2A).27 The stomach resection is usually restricted to the antrum, and a truncal vagotomy is often associated. A considerable amount of remaining stomach with refluxed bile is observed endoscopically. The gastroduodenostomy is found toward the greater curvature. A prominent fold representing the closed part of the stomach is often observed along the lesser curvature ending at the gastroduodenostomy. A mucosal pattern change from gastric folds to flat duodenal surface indicates the anastomosis site. The duodenum is rectified, and the circular folds of the second portion are close to the anastomosis because of the partial resection of the bulb. Major and minor papillae appear to be more proximal in the duodenum than in a patient with intact anatomy.
Billroth II
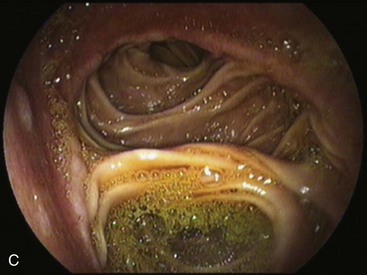
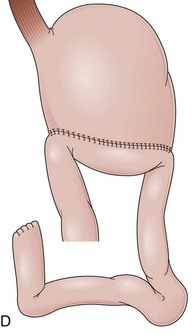
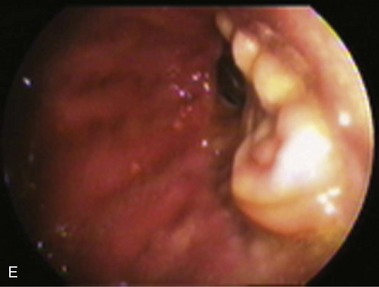
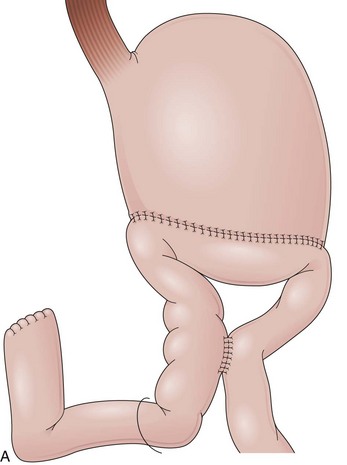
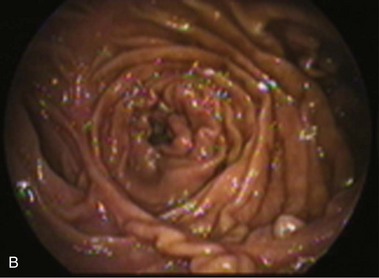
In a Billroth II reconstruction after a partial gastrectomy, the duodenal stump is closed and a gastrojejunostomy is created (Fig. 11.2B). This type of reconstruction, commonly used for complicated ulcer disease in the past, is now used more often in the treatment of gastric neoplasia in which extensive resections are required. The remaining stomach is variable in length allowing the retroflexion maneuver if a long segment is present. The gastric remnant usually contains frothy bile and mucosal erythema from the alkaline reflux.28 The gastrojejunostomy is located at the distal end of the stomach where two stomal openings corresponding to an end-to-side anastomosis can be identified (Fig. 11.2C).
Several surgical techniques are employed to perform the gastrojejunostomy leading to distinct endoscopic presentations. The chosen technique depends on surgeon preference, and there is no consensus for the ideal one. The gastrojejunostomy can vary in the size of the anastomosis, in the orientation of the jejunal loop to the stomach, and in the position of the anastomosis to the transverse colon. If the whole length of the transected stomach is anastomosed to the jejunum (oralis totalis or Polya), several rows of jejunal folds are observed between the two stomal openings (Fig. 11.3A). Conversely, if only a segment of the transected stomach is anastomosed to the jejunum (oralis partialis or Hoffmeister), few or no folds are evident. In this case, the stomach is partially closed, always from the lesser curvature, to reduce the diameter of the anastomosis, which is observed toward the greater curvature. Some surgeons attach the jejunal limb to the suture line that is closing the stomach to prevent dehiscence when performing an oralis partialis anastomosis (Fig. 11.3B).29 In this case, a sharp angulation might be negotiated to enter the corresponding jejunal limb, and a prominent fold may be seen emanating from the lesser curvature to the anastomosis. The small anastomosis diameter in association with the sharp angulation of this type of reconstruction may make the anatomy difficult to define endoscopically.
Gastrojejunostomies performed with staplers are usually oralis partialis. In some cases, the stomach is completely closed at the distal end, and the gastrojejunal anastomosis is performed with a linear or a circular stapler in a side-to-side fashion at the posterior wall, 2 cm proximal to the end of the stomach.30 When observed endoscopically, however, this side-to-side anastomosis is almost indistinguishable from a short end-to-side anastomosis. The jejunum can be anastomosed to the stomach with the afferent limb attached to the greater curvature (isoperistaltic) or to the lesser curvature (antiperistaltic). The afferent limb refers to the jejunal limb that is in continuity with the duodenum, whereas the efferent limb refers to the one that leaves the stomach toward the distal jejunum. The two stomal openings observed endoscopically may represent the afferent or efferent limb depending on how the reconstruction was performed (Fig. 11.3C and D). If the reconstruction is isoperistaltic, the opening linked to the greater curvature corresponds to the afferent limb. If the reconstruction is antiperistaltic, the opening linked to the greater curvature corresponds to the efferent limb. Usually the stomal opening linked to the lesser curvature is more difficult to access with the endoscope because of the relative verticalization of the anastomosis (Fig. 11.3E).31
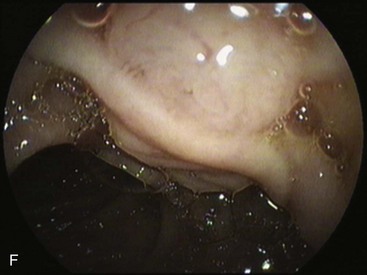
Gastrectomies usually include the lesser more than the greater curvature in the resection. In addition, the information from surgical notes about the type of reconstruction, peristalsis, and bile flow might help to define the limbs endoscopically. On careful observation of the anastomosis, bile may be seen coming predominantly from the afferent limb. Introducing the endoscope through this opening should reveal an increasing volume of bile as the endoscope advances toward the bulb, although bile may also be observed in the efferent limb. Visible peristaltic waves advancing away from the endoscope suggest that the instrument is in the efferent limb. When the duodenal stump is reached, the flat mucosa of the residual bulb with a scarlike deformity in a cul-de-sac can be identified. A careful withdrawal of the endoscope exposes the major papilla, usually located at the right upper quadrant on the monitor screen (Fig. 11.3F).
In patients with Billroth II anatomy, the papilla is rotated 180 degrees in the endoscopic visual field. This “upside down” position requires distinct techniques to perform endoscopic retrograde cholangiopancreatography (ERCP), including dedicated sphincterotomes, needle-knife cut technique over the stent, or balloon dilation of the papilla.32–36 If the duodenal stump cannot be identified, the endoscope should be withdrawn, and the other limb should be intubated as far as possible. Fluoroscopic guidance may indicate that the efferent limb has been entered when the instrument is seen to pass deep into the pelvis. Conversely, passage of the endoscope into the right upper quadrant toward the liver or previous cholecystectomy clips suggests entry into the afferent limb.37
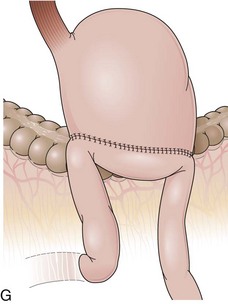
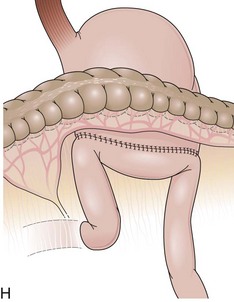
The length of the afferent limb also varies depending on the surgical technique. The afferent limb naturally fixed at the ligament of Treitz and surgically fixed to the stomach should be tensionless but not redundant. There are two ways to position the afferent limb in relation to the transverse colon during a Billroth II reconstruction. If an antecolic anastomosis is performed, the gastrojejunostomy is placed anterior to the transverse colon (Fig. 11.3G). Antecolic reconstructions frequently have long afferent limbs because of the distance between the ligament of Treitz and the remaining stomach, over the mesocolon, omentum, and transverse colon. Conversely, retrocolic reconstructions are performed through an opening in the transverse mesocolon, shortening the distance between the ligament of Treitz and the remaining stomach (Fig. 11.3H).38,39 Antecolic and retrocolic anastomoses are similar endoscopically except for the unspecific observation obtained from the length of the limbs. Caution should be taken if a percutaneous endoscopic gastrostomy is indicated for a patient with a previous partial gastrectomy and retrocolic reconstruction.
Billroth II reconstruction can be associated with a side-to-side jejunojejunostomy, referred to as the Braun procedure (Fig. 11.4A).40 This procedure creates an anastomosis between the afferent and the efferent limb to divert bile from the gastric remnant and to release the pressure of the afferent limb, supposedly preventing duodenal stump fistula.41 The Braun anastomosis is performed 10 to 15 cm distal to the gastrojejunostomy and requires a longer afferent limb to accommodate the jejunojejunostomy.42 Endoscopically, the gastrojejunostomy is similar to a standard Billroth II. Frothy bile is present in the stomach because the Braun procedure only partially diverts biliopancreatic fluids from the gastrojejunostomy. After advancing the endoscope through either opening of the gastrojejunostomy, the side-to-side Braun anastomosis can be found in the afferent and efferent limb, and three openings can be noted (Fig. 11.4B). One leads to the distal jejunum, one leads to the afferent limb, and the third one leads back to the stomach. A complete reverse intubation of the stomach may be carried out through the loop created with the Braun anastomosis. The same anatomic landmarks described for other Billroth II procedures are helpful in directing the endoscope through the limbs. However, a trial-and-error approach may be necessary ultimately to reach the duodenal stump.
A higher rate of perforation has been reported during ERCP while traversing the afferent limb compared with standard ERCP, particularly when a stiff therapeutic duodenoscope is used.43,44 The Braun procedure has also been associated with perforations during ERCP. The use of a forward-viewing endoscope in these patients can reduce the risk of jejunal perforations.45 The ability to use a duodenoscope elevator may increase the success of the procedure, and a flexible diagnostic duodenoscope may be safer than a stiff therapeutic instrument. If the papilla cannot be located with a side-viewing endoscope, a forward-viewing endoscope should be attempted and vice versa. Patients with an excessively long afferent limb may require longer endoscopes to reach the papilla.
Roux-en-Y Gastrectomy
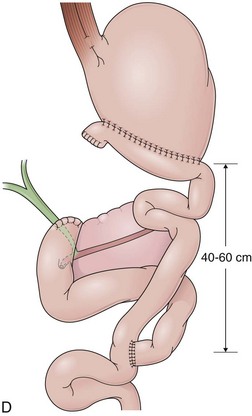
In a Roux-en-Y reconstruction, the jejunum is transected close to the ligament of Treitz, creating two distinct segments. The distal segment is sutured to the gastric remnant (gastrojejunostomy) becoming the efferent limb. The proximal segment is sutured to this efferent limb (jejunojejunostomy) approximately 40 cm below the gastrojejunostomy (see Fig. 11.2D). The proximal segment is called the afferent limb, which connects the duodenum to the efferent limb instead of the stomach as in Billroth II reconstructions. The Roux-en-Y prevents biliopancreatic fluids from refluxing into the stomach in patients who have undergone gastric resection. It can be performed as the initial reconstruction after a gastrectomy or as the treatment for postgastrectomy syndrome resulting from a previous Billroth II reconstruction.46–48 Truncal vagotomy is commonly performed in association with Roux-en-Y to prevent peptic ulcers in the efferent limb, which is no longer washed by the alkaline contents of the biliopancreatic fluid.49
In effective Roux-en-Y reconstructions (Fig. 11.5), the remnant stomach is completely clean of bile (see Figs. 11.3A and B and 11.5A and B






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


