which usually tapers towards the anal verge. A rectal bar representing a more prominent longitudinal fold may be visualized along the anterior rectal wall (see Figure 6.9). A subtle, small pseudopolypoid lesion may be visualized along the posterior rectal wall on the 2D views at the point of anterior angulation of the rectum (see Figure 6.10).
TABLE 6.1 Pitfalls on Virtual Colonoscopy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The appendix may be partially or completely inverted. Use of the older inversion-ligation technique for appendectomy, which is not often used currently, will result in an appendiceal stump that may simulate a polyp.12 If a potential polyp is identified on axial or 3D views, the reader should refer to the coronal or sagittal reformats to attempt to identify the appendix and the relation of the appendix, if present, to the lesion. History of prior appendectomy is important to obtain. An appendicolith is often also readily identifiable on 2D views. An inverted or intussuscepted cecal diverticulum has also been reported to simulate a pedunculated polyp on CT scan.13
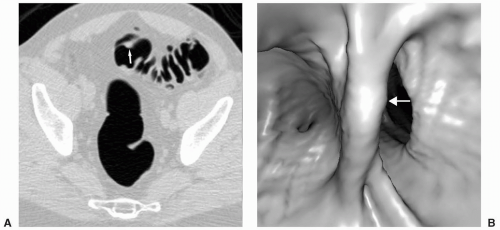 FIGURE 6.1 Bulbous Fold: Axial image (A) reveals a polypoid lesion on a fold. The 3D endoluminal view (B) demonstrates a bulbous fold. No polyp was identified on colonoscopy. |
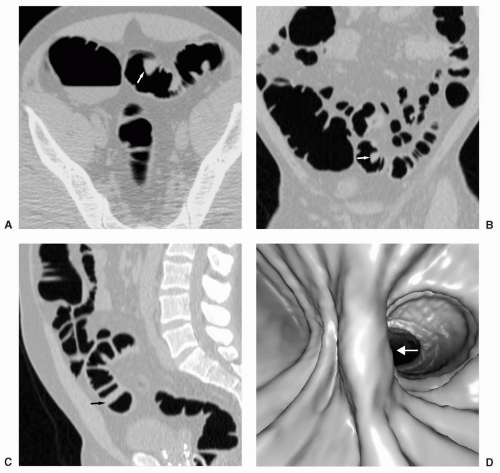 FIGURE 6.2 Bulbous Fold: Axial supine image (A) and coronal reformat (B) reveal a homogeneous soft tissue density lesion in the sigmoid. The sagittal reformat (C) reveals a bulbous fold, which is also seen on the 3D image (D). HINT: Note the polygonal appearance of the lesion on the first two views, which is not consistent with a true polyp. |
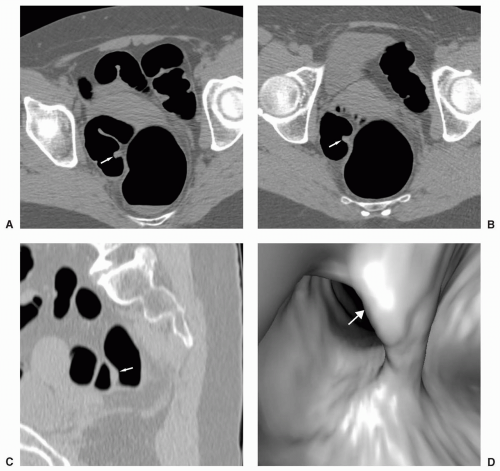 FIGURE 6.3 Bulbous Fold: Both the axial supine (A) and prone (B) images reveal a nonmobile homogeneous pseudopolypoid lesion. The sagittal view (C) and the 3D endoluminal view (D) demonstrate a bulbous fold. |
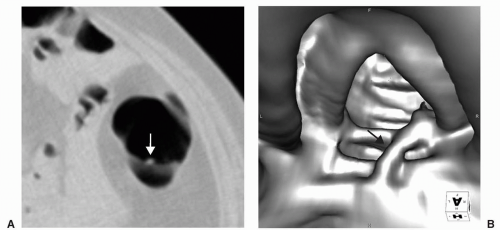 FIGURE 6.4 Crossing Fold: Axial view (A) shows a small polypoid-appearing lesion on the middle of a fold. The 3D endoluminal view (B) shows an atypical fold that crosses the other haustral folds. |
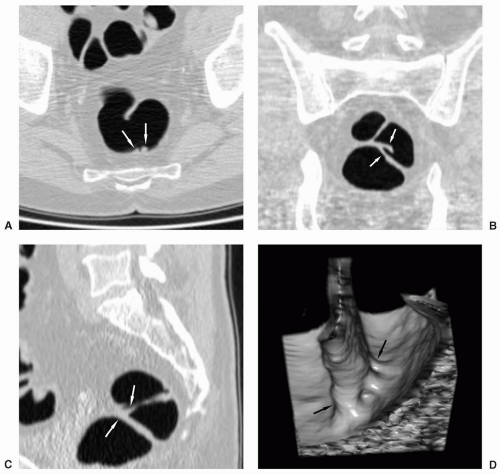 FIGURE 6.5 Confluence of Folds, Rectum: Axial image (A) shows two small pseudopolypoid lesions along the posterior wall. The coronal (B) and sagittal (C) reformats reveal that these represent the confluence of folds. The 3D cube view (D) also shows this well. |
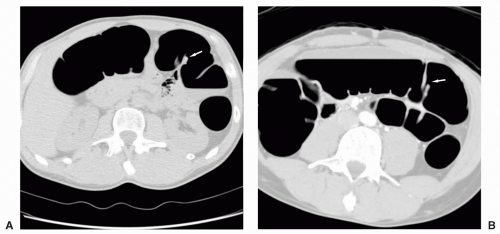 FIGURE 6.6 Confluence of Folds, Transverse Colon: Axial supine image (A) reveals a possible polyp. Images (B) and (C) represent consecutive slices from the axial prone series showing that this “lesion” represents a confluence of folds. The 3D endoluminal image (D) also shows folds converging. (Views C and D are on next page.) |
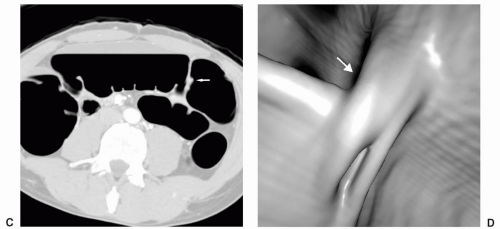 FIGURE 6.6 (Continued). |
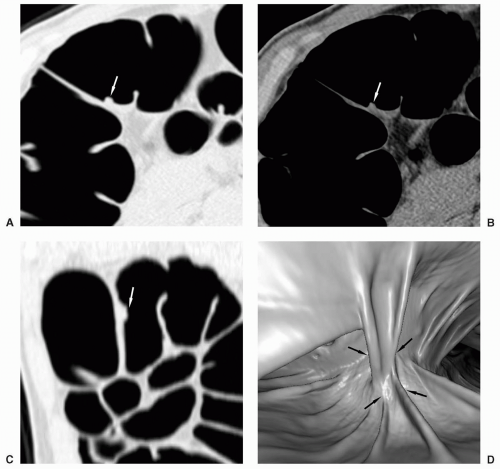 FIGURE 6.7 Complex Folds, Splenic Flexure: Axial images in colon (A) and abdominal (B) windows show a homogeneous pseudopolypoid lesion on a fold. The sagittal reformat (C) also shows the lesion. The 3D endoluminal view (D) shows a complex series of folds in an area of curvature. |
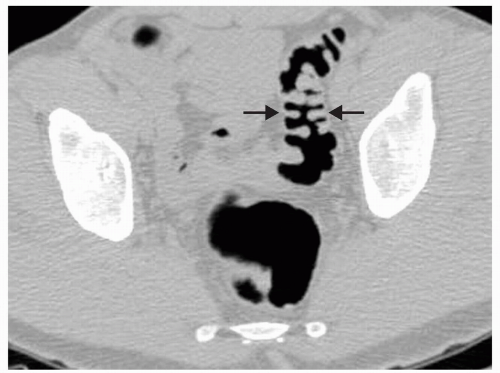 FIGURE 6.8 Kissing Folds: Axial image shows enlarged folds that may simulate polyps that extend towards the middle present in a poorly distended sigmoid. |
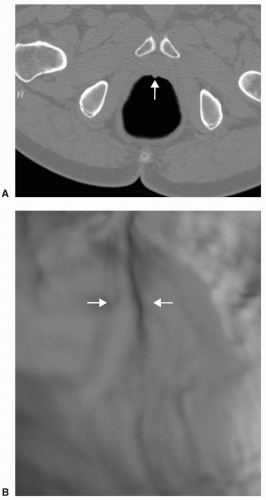 FIGURE 6.9 Anterior Rectal Bar: A small pseudopolypoid lesion is present along the anterior rectal wall on the axial image (A). This correlates with a prominent fold in the same location on the 3D endoluminal view (B). |
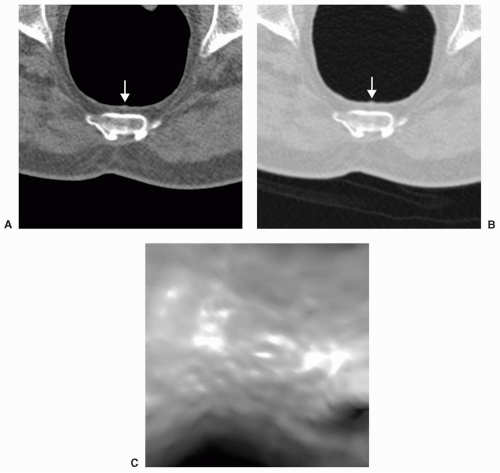 FIGURE 6.10 Posterior Rectal Wall Pseudopolyp: A minimal small protrusion can be seen on the axial images in abdominal (A) and colon (B) windows along the posterior rectal wall. No lesion is identified on the 3D view (C). This finding has been described as the result of anterior angulation of the rectum. |
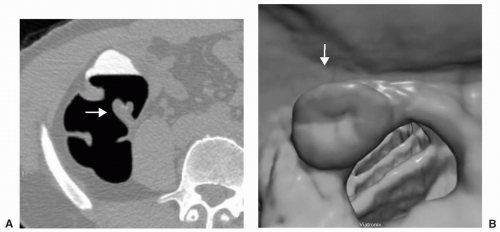 FIGURE 6.11 Normal Ileocecal Valve: Axial (A) and 3D endoluminal (B) views show the typical appearance of the ileocecal valve as rounded or ovoid with a central depression or pit. |
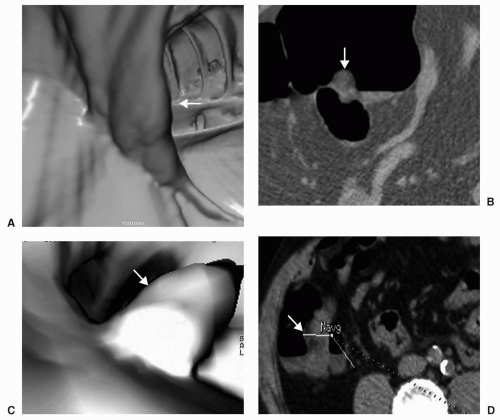 FIGURE 6.12 Lipomatosis of the Ileocecal Valve: When the ileocecal valve becomes infiltrated with fat, the central depression may not be as evident on the 3D endoluminal view (A). The axial view demonstrates the fatty density of the valve (B). In another patient lipomatosis causes the ileocecal valve to enlarge and appear mass-like on the 3D endoluminal view (C) and on the axial view (D). |
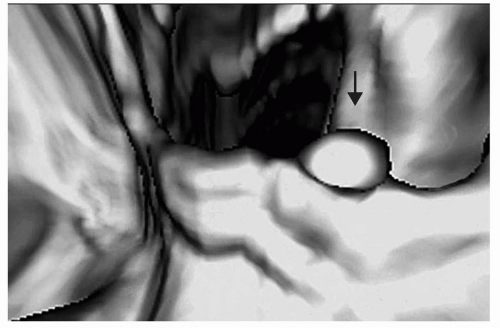 FIGURE 6.13 Polyp on Ileocecal Valve: The ileocecal valve is covered by colonic mucosa and polyps and carcinoma can develop on the valve. 3D endoluminal view shows a polyp on the ileocecal valve. |
However, if malrotation occurs without clinical consequence, patients may present for CTC because of failed colonoscopy (see Figure 6.19). Findings that suggest malrotation are failure of the duodenum to cross midline to the left, vertical, or reversed orientation of the superior mesenteric vessels, and unusual position of the cecum and large bowel, or small bowel.16,18
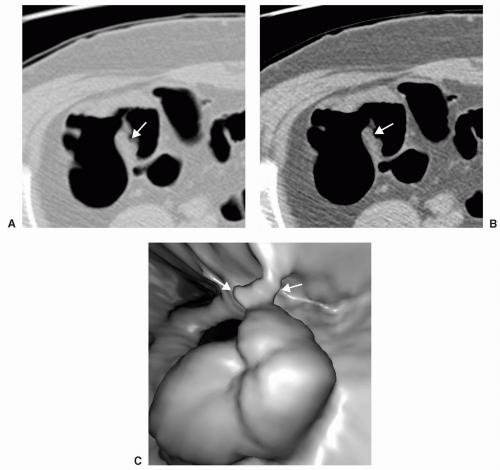 FIGURE 6.14 Stool on Ileocecal Valve: Prone axial view in colon (A) and abdominal (B) windows shows an angulated contour of the ileocecal valve. 3D endoluminal view confirms irregular surface of the valve due to adherent stool (C). |
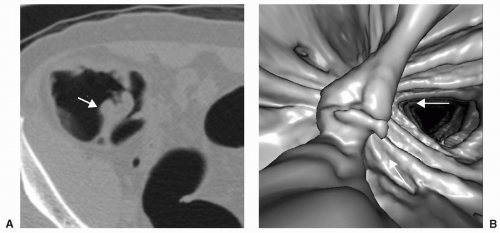 FIGURE 6.15 Stool on Ileocecal Valve: Axial view (A) shows an extra “lip” on the ileocecal valve. 3D endoluminal view (B) shows an irregular contour of the ileocecal valve with a linear and lobulated appearance due to adherent stool. |
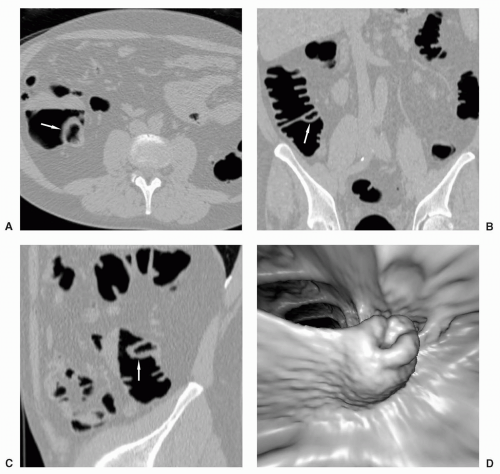 FIGURE 6.16 Prolapsed Terminal Ileum: Axial view (A), coronal reformat (B) and sagittal reformat (C) demonstrate an air-distended terminal ileum (white arrow) bulging into the right colon, causing an elongated appearance of the ileocecal valve on the 3D endoluminal view (D). |
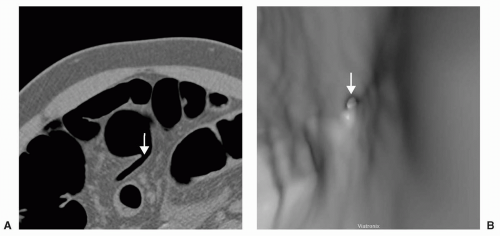 FIGURE 6.17 Appendiceal Orifice: Axial view (A) shows an air-filled appendix extending from the cecal tip. The open appendiceal orifice appears as a dark ring on the 3D endoluminal view (B) similar to a diverticulum. |
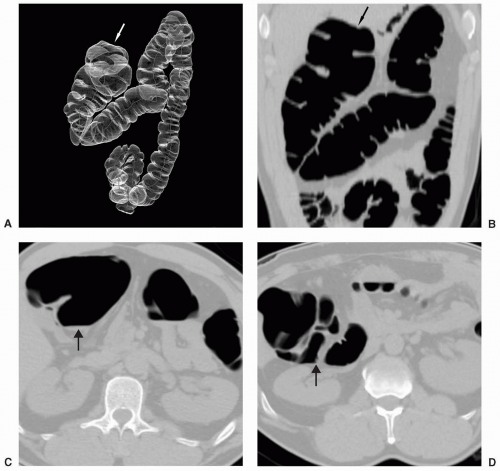 FIGURE 6.18 Cecal Bascule: The cecum rotates superior and anteromedial to the ascending colon. These patients can present for CTC after incomplete colonoscopy. The 3D transparency view (A) and the coronal multiplanar reformat (B) are best for showing the course of the right colon and the location of the cecum relative to the ascending colon. The axial supine (C) and prone (D) views demonstrate the high location of the cecum. |
epigastric vessels (see Figure 6.21). Direct inguinal hernias occur through a weakened area of the transversalis fascia within an area referred to as Hesselbach’s triangle. The sac of a direct hernia is typically located medial to the inferior epigastric vessels. In a study by Sosna et al. four of seven patients who developed colonic perforation at CTC had left inguinal hernias that contained sigmoid colon.19 It was postulated that incarceration of the sigmoid occurred at the hernia site which was likely caused by the insufflation of air. Practice patterns were changed so that in patients with known inguinal hernia special attention was given to the inguinal region during the insufflation process and if there was increase in size of the hernia sac, air insufflation was halted. Patients with less common hernias that may involve the colon, such as Spigelian hernias (anterior abdominal wall along lateral margin of the rectus abdominus muscle), internal hernias, or hernias occurring as a result of trauma or other surgery, may present for CTC due to incomplete colonoscopy or may be detected incidentally on CTC (see Figure 6.22).
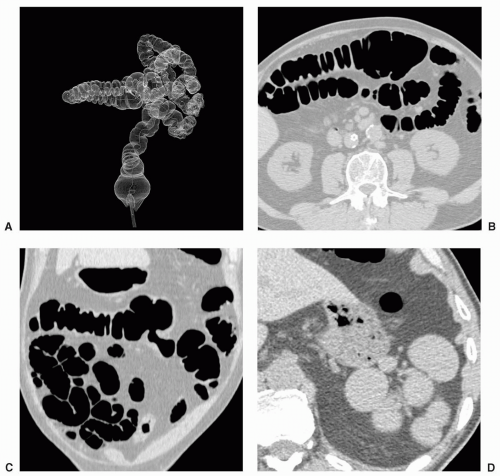 FIGURE 6.19 Polysplenia: 3D transparency view (A) shows malrotation of the colon with the right colon located anterior to the transverse colon. Axial supine image (B) demonstrates the cecum in the left upper quadrant and the acute bend of the colon in the right upper quadrant causing for failed colonoscopy. Coronal multiplanar reformat (C) demonstrates small bowel loops in the right lower quadrant. The axial supine image in abdominal window (D) demonstrates multiple small spleens in this patient with previously undiagnosed polysplenia. |
CTC has not been advocated for patients with a colostomy following APR. In a study by Burling et al. perforation of a rectal stump occurred in a patient who underwent CTC inadvertently because adequate surgical history was not communicated or elicited.21 Perforation occurred at the suture line at the apex of the rectal stump (patient presumably had prior LAR). This emphasizes the importance of obtaining a complete surgical history before performing CTC.
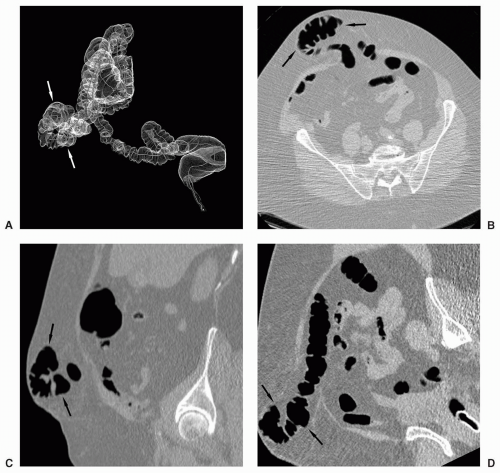 FIGURE 6.20 Ventral Hernia: 3D transparency view (A) from a patient referred for an incomplete colonoscopy shows an abnormal position of the transverse colon. Axial image in colon window (B) shows herniation of the transverse colon into the fat of the anterior abdominal wall. Sagittal (C) and parasagittal reformats (D) shows exact location of the herniated transverse colon and easy evaluation. |
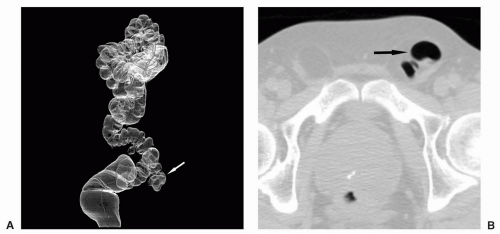 FIGURE 6.21 Inguinal Hernia: 3D transparency view (A) shows a left inguinal hernia containing sigmoid colon. Axial (B), sagittal (C), and coronal (D) reformats delineate the portion of the sigmoid located in the hernia sac and allows for evaluation for lesions. (Views C and D are on next page.) |
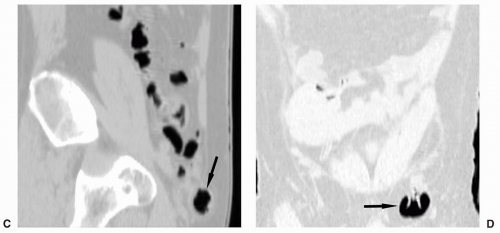 FIGURE 6.21 (Continued). |
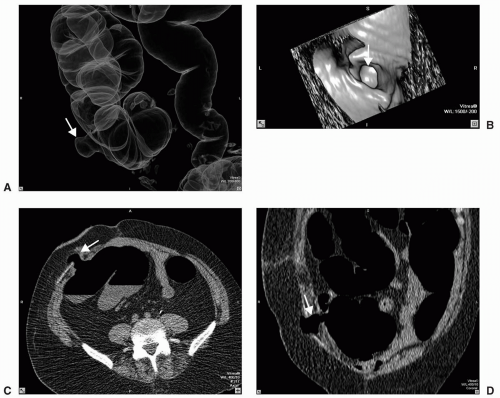 FIGURE 6.22 Stomal Hernia: 3D transparency view (A) shows focal herniation of ascending colon through an old ostomy site which appears as a large black ring simulating a diverticulum on the 3D endoluminal view (B). The axial (C) and coronal reformat (D) shows clearly the protrusion of a knuckle of ascending colon through the abdominal wall defect. |
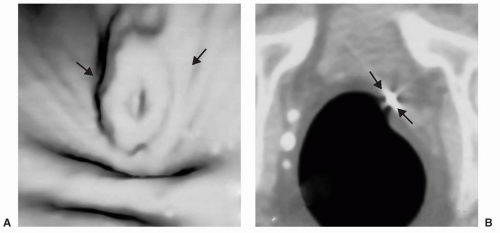 FIGURE 6.23 Postsurgical Deformity: 3D endoluminal view (A) reveals an ovoid lesion with a central defect which is seen to represent deformity with puckering of the colon wall due to a surgical clip on the axial view (B). |
center of the cecum to the ICV. Any degree of rotation of this line was interpreted as axial mobility. Rotation that could impact the diagnosis was found to occur in 9/21 (43%) cases with an average rotation of 78.9 +/−27.4 degrees. In the 12 cases that did not pose a diagnostic dilemma, the average rotation was still 22.5+/−12 degrees. In addition, the main axis of rotation was varied, occurring predominantly in coronal (6 cases), sagittal (4 cases), or axial (11 cases) planes. It was concluded that rotation of the colon occurs frequently, is geometrically complex, and occurs in several planes. Multiplanar reformatted views are helpful when solid stool is suspected in the cecum to assess for rotation.
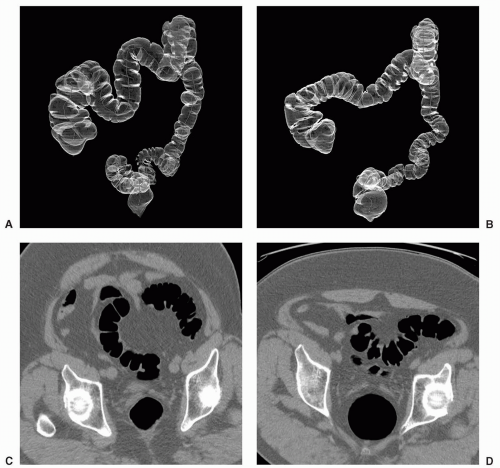 FIGURE 6.24 Sigmoid and Transverse Colon Mobility: 3D transparency views in the supine (A) and prone (B) positions show straightening of both the sigmoid and transverse colon. Axial views in the supine (C) and prone (D) positions shows relative movement of a portion of the sigmoid colon more posterior. |
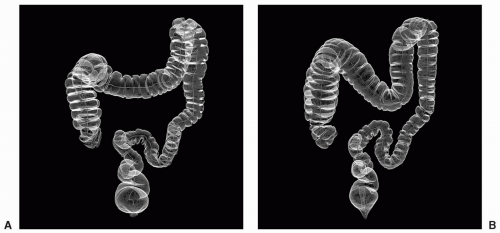 FIGURE 6.25 Sigmoid and Transverse Colon Mobility: 3D transparency views in the supine (A) and prone (B) positions show straightening of the sigmoid colon in the prone position but the transverse colon moves inferiorly. This is also depicted on the coronal reformats in the supine (C) and prone (D) positions. |
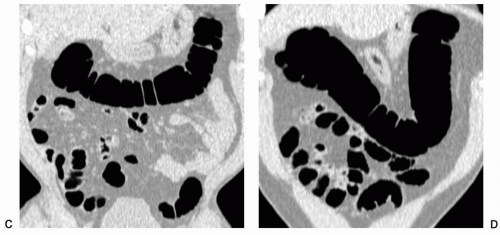 FIGURE 6.25 (Continued). |
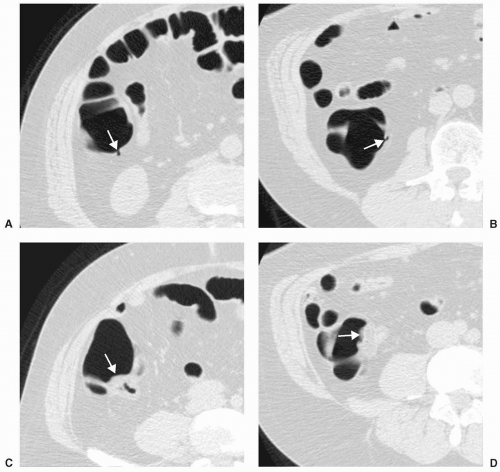 FIGURE 6.26 Right Colon Mobility: Note the position of the same diverticulum located posterior on the supine view (A) and medially on the prone view (B). The position of the ileocecal valve posterior on the supine view (C) and located medially on the prone (D) view confirms rotation of the ascending colon and cecum. |
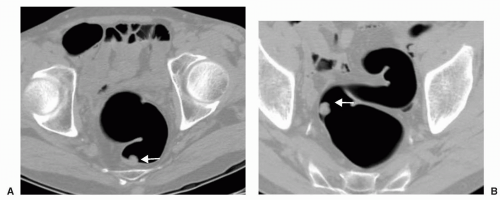 FIGURE 6.27 Mobile Sigmoid with Polyp: Supine axial view (A) shows a polyp along the posterior wall of the distal sigmoid colon. The stalk of this pedunculated polyp is seen on the prone view (B)
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|





