28 Patient preparation and principles of sedation in gastrointestinal endoscopy
Case
A 67-year-old male with a past history of mitral valve stenosis and insulin-dependent diabetes mellitis with moderate renal impairment requests his primary care physician to organise colon cancer screening. An open-access colonoscopy is arranged.
Introduction
This chapter deals with several of the most important aspects of providing a safe endoscopic practice: preprocedure patient assessment, management of anticoagulation, antibiotic prophylaxis and intraprocedural sedation.
Preparing Patients for Endoscopy
Endoscopic retrograde cholangiopancreatography
Patients undergoing ERCP will be exposed to ionising radiation. Therefore women of childbearing age should have pelvic shielding during the procedure. If there is any possibility of pregnancy a serum or urinary β-human chorionic gonadotropin should be checked. Contrast medium in the bowel lumen can obstruct views of the biliary system, so patients who have recently had a CT scan with contrast or a barium study should have a plain abdominal x-ray to ensure the biliary system is not obscured. As iodinated contrast is used to inject into the biliary system, a history of iodine allergy or hyperthyroidism should be elicited, though history of a contrast allergy is not an absolute contraindication as the risk of an allergic reaction during ERCP is extremely low. Patients with biliary obstruction should receive prophylactic antibiotics prior to the procedure. Due to the risk of bleeding with sphincterotomy of the ampulla of Vater, elective patients on clopidogrel should ideally withhold this medication for 7–10 days if feasible. The risk is lower with aspirin (all therapeutic endoscopy can be performed on aspirin). Discussion with the patient’s cardiologist is prudent if there is uncertainty whether it is safe to withhold these medications. Coagulopathy should be reversed if present; patients on warfarin may need to change to low-molecular-weight heparin prior to the procedure depending upon the indication. The decision when to reinstitute anticoagulant therapy following therapeutic procedures such as ERCP and colonic polypectomy is a difficult one and should be individualised in consultation with the patient’s cardiologist.
Antibiotic prophylaxis
Advice regarding antibiotic prophylaxis prior to endoscopic procedures was significantly updated in American Society for Gastrointestinal Endoscopy guidelines (2008) based on the recognition from the American Heart Association that bacterial endocarditis from endoscopic procedures was exceedingly rare. For the majority of patients undergoing endoscopic procedures, including those with prosthetic heart valves or congenital cardiac abnormalities, antibiotic prophylaxis to prevent bacterial seeding was no longer recommended. There are however, certain situations in which the risk of infective complications (which may be local rather than systemic) is increased and antibiotics are warranted; these are listed in Box 28.1.
Box 28.1 Antibiotic prophylaxis for endoscopy
All patients prior to insertion of percutaneous endoscopic gastrostomy
All patients with cirrhosis with acute GI bleeding (intravenous ceftriaxone from admission)
Disease-specific issues
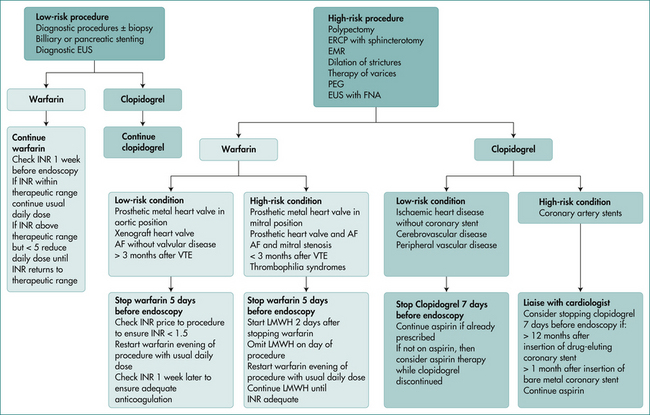
Patients can take their normal medications several hours prior to the procedure with a sip of water. The management of patients taking antiplatelet agents or anticoagulants is a complex issue, and should be in accordance with published guidelines. These guidelines take into account whether the procedure is elective or an emergency procedure, the indication for the antiplatelet agent or anticoagulant, and the bleeding risk related to the procedure. A suggested algorithm for management of patients requiring anticoagulation is outlined in Figure 28.1.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


