Departments of Pathology and *Medicine, University of Maryland School of Medicine, Baltimore, Maryland 21201
INTRODUCTION
Continuous clinical, surgical and pharmacological advances in renal transplantation depend heavily on the routine analysis of graft biopsies. Many therapeutic decisions are based on the biopsy findings. Of the tens of thousands of scientific articles dealing with renal transplantation, one fifth include clinicopathological correlations.
Biopsies cannot be interpreted in isolation. Adequate clinical information is necessary for an accurate pathological diagnosis. The subtleties of clinical and pathologic diagnosis need to be understood by the clinician and pathologist if the most appropriate care is to be delivered to the transplant recipient. Furthermore, if the pathologist and the treating physician have the opportunity to look at the biopsy together, invaluable information may be exchanged between them. This chapter has been prepared for the nonpathologist professionals involved in the treatment of renal transplant patients, in an attempt to help them become familiar with the main histopathological concepts.
SPECIMEN ADEQUACY
Due to the fact that many pathological processes involve the kidney allograft in a patchy, random manner, the sensitivity of the biopsy depends on the amount of tissue available for evaluation. To diagnose or rule out acute allograft rejection with some degree of certainty, it is necessary to evaluate a sample of renal cortex containing a sufficient number of glomeruli and arteries. According to the Banff schema (see below) a specimen must contain ten or more glomeruli and at least two arteries to be considered adequate. Ideally, two separate areas of cortex should be present, either in the same core or in two separate cores (1). Evaluation of two tissue needle cores is desirable to achieve a sensitivity of 99% for the diagnosis of acute rejection. This is in contrast to a sensitivity to 90% for a single core (2,3). The amount of tissue required also depends on the biopsy indication. There are clinical situations in which enough tissue material must be obtained to allow for the performance of ancillary studies such as immunofluorescence and electron microscopy. This is particularly the case in patients being evaluated for a glomerular disease.
TABLE 31.1.Clinical information
Time posttransplant
Type of transplant: living donor or cadaveric
Peritransplantation surgical complications
Indication for biopsy
Increase in serum creatinine (rapid, slow)
Type of immunosuppression
Changes in immunosuppression
Use of nephrotoxic drugs
Proteinuria
Infection
Dehydration
Renal artery stenosis
Abnormal imaging studies (i.e., hydronephrosis)
Acute cellular rejection is largely a cortical event. Significant rejection may be missed in biopsies that contain predominantly medullary tissue. Biopsies containing only medulla are in general considered inadequate because in those samples, acute allograft rejection will be missed or underestimated in half the cases (4). On the other hand, examination of renal medulla may be sufficient to diagnose other pathological entities (i.e., acute pyelonephritis, polyomavirus nephropathy).
For an optimal histopathological interpretation, it is very important that all pertinent clinical information is provided to the pathologist. Table 31.1 lists the most important clinical information useful in the interpretation of a renal transplant biopsy.
ROUTINE AND MAIN ANCILLARY STUDIES
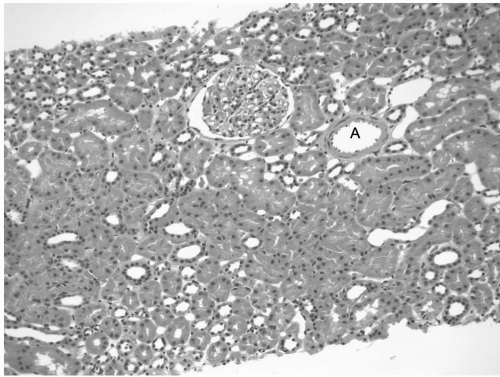
Light microscopic evaluation of renal biopsies includes the performance of hematoxylin- and eosin-stained sections (Fig. 31.1), as well as additional routinely used special stains. The most important special stains are the PAS (periodic acid Schiff), silver (periodic acid methenamine silver [PAMS]) and Massons trichrome stains (1). Table 31.2 summarizes the main morphological features identified with each of these stains.
Several other special stains are performed as needed. Immunohistochemical and in situ hybridization techniques for the identification of a variety of infectious organisms are available. Specifically, the stain for SV40 is used for the diagnosis of polyomavirus nephritis due to its cross reactivity with the BK and JC viruses. Molecular studies, particularly polymerase chain reaction (PCR) are also useful to demonstrate the presence of infectious organisms in tissue samples (5), although these studies are not routinely used for diagnostic purposes.
FIG. 31.1. Hematoxylin and eosin stain of a normal kidney transplant (protocol biopsy of a well-functioning graft). There is no inflammation. The tubules are “back to back” with no significant intervening connective tissue (inconspicuous interstitium). A: Normal artery. Note the thin wall and the widely open lumen.
TABLE 31.2.Routinely* used special stains: main diagnostic value
Periodic acid-Schiff stain*
Tubules: tubulitis, destruction of tubular basement membranes, thickening of basement membranes (atrophy)
Glomeruli: glomerulitis (mononuclear cells in capillaries), reduplication of basement membranes (transplant glomerulopathy), increase in mesangial matrix, hyalinosis
Vessels: hyalinosis
Other: identification of fungal organisms
Silver stain*
Tubules: tubulitis, destruction of tubular basement membranes, thickening of basement membranes (atrophy)
Glomeruli: glomerulitis (mononuclear cells in capillaries), reduplication of basement membranes (transplant glomerulopathy), increase in mesangial matrix
Epstein-Barr virus latent membrane protein (LMP-1)
Epstein Barr encoded RNA
Adenovirus
Immunofluorescence immunohistochemical stains for immunoglobulins and complement components are routinely used in the evaluation of glomerular diseases in renal transplants in the same manner as it is done in native kidneys. It is important to remember that the immunofluorescence technique can be applied only to tissues that are fresh-frozen (not fixed in formaldehyde). Stains for immunoglobulins and complement components are also used when humoral rejection is suspected. In typical cases of humoral rejection (i.e., hyperacute rejection), deposition of IgG and complement components is seen in vascular walls. Some morphologically subtle forms of humoral rejection require the use of special stains for their diagnosis. The C4d stain identifies an important subset of antibody-mediated rejections. C4d is a complement split product that remains covalently bound to target structures after complement activation has occurred, allowing for its recognition in tissue sections. This is in contrast to most products of complement activation that are immediately degraded. Deposition of C4d in intertubular capillaries and other vascular structures identifies ongoing humoral rejection that would otherwise escape identification (6). Due to this reason, immunohistochemical stain for C4d is now considered part of the routine biopsy workup in patients with early allograft dysfunction (see below humoral rejection). The C4d stain can be performed in fresh-frozen as well as formalin-fixed tissue.
Evaluation of routine urine cytology is an inexpensive and simple tool to determine if a patient has polyoma virus replication in the urinary tract. The infected cells that shed in the urine are identified by their large size and typical intranuclear inclusion (“decoy cells”). The large majority of transplant recipients have BK virus infection that is latent. Up to 30% of patients will on occasion shed infected cells into the urine. Only a small portion of these patients will have active nephropathy identified by biopsy. On the other hand, persistent urinary shedding of decoy cells is strongly associated with viral nephropathy (7,8). Decoy cells in urine precede the histological evidence of nephritis. Of even more importance is the fact that a negative urine cytology has a negative predictive value for viral nephritis of nearly 100% (9). Quantitative PCR for BK virus in urine is also used for screening and follow-up of renal transplant patients in a similar manner as urine cytology.
MORPHOLOGICAL FEATURES OF ACUTE REJECTION
Transplant rejection occurs in several forms including, hyperacute, acute cellular, acute humoral, and chronic rejection/graft sclerosis. Although these various forms of rejection can overlap, there are distinct clinical patterns in their respective presentations. An appreciation of these patterns will aid the clinician in identifying patients requiring biopsy and in interpretation of the histological findings. Hyperacute rejection is immediate and related to preexisting antibody to allograft tissue. Advances in tissue typing have largely eliminated hyperacute rejection; however, it may still be seen in highly sensitized recipients. Acute cellular and humoral rejections have a peak incidence in the first few months following transplantation, and they may coexist. These forms of rejection may occur anytime following transplantation and may occur late in patients noncompliant with immunosuppressive medications. Unrecognized and untreated acute rejection results in a rapid and progressive loss of transplant function. Chronic rejection is generally a later event, often presenting a year or more following transplantation. It is manifested as a relatively slow progressive loss of transplant function.
The pathological diagnosis of rejection is based on the presence of a constellation of features indicating immune activation and associated tissue damage (3).
Acute (Active) Cellular Rejection
Acute cellular rejection is a T-cell-mediated reaction to donor-specific antigen. It has tubulointerstitial, vascular and rarely glomerular manifestations.
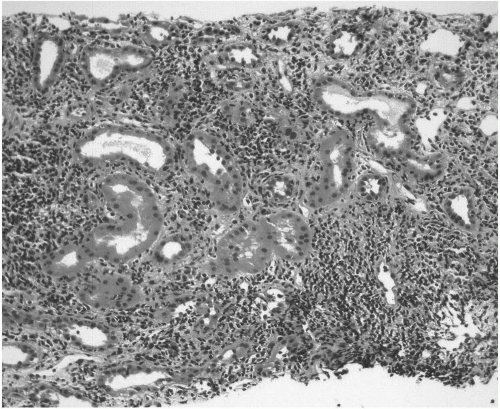
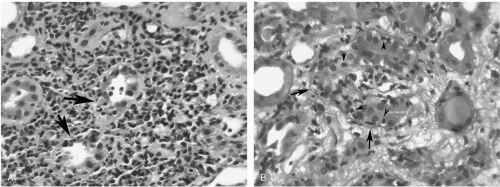
The tubulo-interstitial inflammatory infiltrates are predominantly composed of mononuclear cells. These consist mainly of lymphocytes and macrophages (Fig. 31.2). Plasma cells, eosinophils and less commonly neutrophils can be present. In the background of interstitial inflammation there is tubulitis. This is defined as infiltration of the tubular epithelium by mononuclear cells, usually T lymphocytes. Tubulitis can be better recognized on PAS and silver stains. These stains clearly demonstrate the location of lymphocytes between the epithelial cells and on the inner aspect of the tubular basement membrane (Fig. 31.3A, B). It is important to remember that inflammation beneath the renal capsule, in areas of scarring (fibrosis), and around large vessels is not considered meaningful for the diagnosis of acute rejection and is ignored in most cases.
FIG. 31.2. Acute cellular rejection. Low power view of a kidney showing prominent interstitial inflammatory infiltrates. The inflammation is predominantly lymphocytic. Tubular inflammation (tubulitis) cannot be appreciated at this power.
FIG. 31.3. Acute cellular rejection. (A) There are prominent mononuclear interstitial infiltrates (lymphocytes, plasma cells, macrophages). There is tubulitis: infiltration of the tubules by the mononuclear cells (arrows). (B) Periodic acid-Schiff stain highlights the outline of the tubular basement membrane (arrows). Numerous lymphocytes (arrowheads) have gone through the basement membrane and are located between the tubular epithelial cells. This is the appearance of tubulitis.
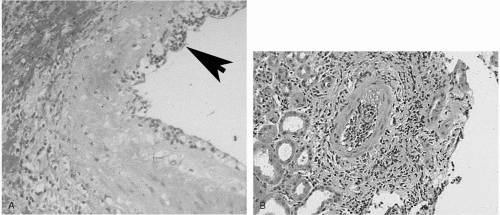
Endothelitis or intimal arteritis is characterized by the accumulation of lymphocytes and macrophages beneath the arterial endothelial lining (Fig. 31.4A, B). This from of arterial inflammation may be an important component of acute cellular rejection. Endothelitis can be so pronounced as to occlude the arterial lumen. Endothelial damage and activation may rarely lead to thrombosis and ischemic complications (patchy coagulation necrosis). Endothelitis is the only lesion specific for acute tubulointerstitial rejection; however, due to sampling, these changes may be absent in core biopsies. On the other hand, tubulointerstitial inflammation is easy to identify but is nonspecific because it is also a feature of infections, allergic nephritis and a variety of other nonspecific processes (see below).
FIG. 31.4. (A) Acute cellular rejection. Endothelitis seen in a segment of an artery. Lymphocytes adhere to endothelial cells and accumulate beneath the endothelial lining (arrow). The wall is also thickened (arterial sclerosis). (B) Another example of endothelitis. The lumen of this artery is occluded by a mixture of inflammatory cells and reactive endothelial cells.
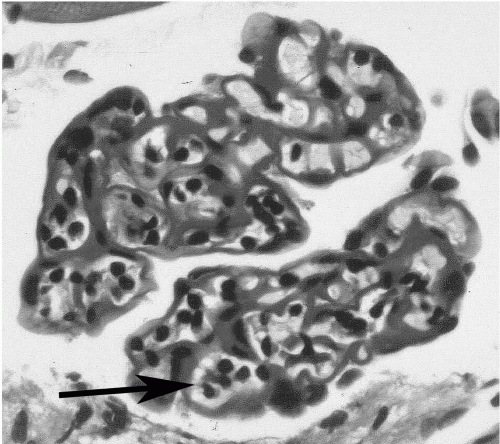
In glomerulitis, a less common manifestation of cellular rejection, the glomeruli show diffuse endothelial swelling with occlusion of the capillary lumen and associated infiltration of T cells and monocytes (10,11) (Fig. 31.5).
FIG. 31.5. Glomerulitis. Periodic acid-Schiff stain highlights the glomerular basement membranes. The capillary lumina contain clusters of lymphocytes (arrow).
Humoral/Antibody-mediated Rejection
The histological features of acute humoral rejection are related to vascular damage resulting from the deposition of alloantibodies occurring in the early post-transplant period (Fig. 31.6A-D)
The most typical and easily recognizable form of humoral (“vascular”) rejection is characterized by fibrinoid necrosis of the arterial smooth muscle and transmural inflammation (arteritis). The arterial walls become bright red and show infiltration by neutrophils and nuclear fragments (Fig. 31.6C). On immunofluorescence stains, the affected blood vessels show deposition of fibrin, immunoglobulin and complement. Because of associated endothelial damage, thrombi can be seen in the lumina of arteries, arterioles and glomerular capillaries. Neutrophils marginate and cluster in the capillary lumina of glomeruli and intertubular capillaries.
In the milder forms of antibody-mediated rejection, the histological findings are minimal, consisting of one or all of the following features: tubular injury (acute tubular necrosis), accumulation of neutrophils in intertubular capillaries and glomeruli, and small vessel thrombosis. The mild forms of antibody-mediated rejection are recognized by the demonstration of C4d in intertubular capillaries. A recent addition to the Banff grading scheme (12) recognizes the heterogeneity of histological findings in antibody-mediated rejection and emphasizes the importance of the C4d staining to recognize its milder forms. Patients with anti-body-mediated rejection present with allograft dysfunction occurring in the early posttransplantation period and have serological evidence of antidonor antibodies. The latter are usually anti-HLA or antiendothelial antibodies (13).
Mixed humoral and cellular acute rejection is not uncommon. C4d staining can identify a humoral component in a significant number of cases that would be diagnosed as pure cellular rejection by morphology alone (6,12, 13, 14).
Hyperacute rejection although very rare, represents the best example of humoral rejection. It occurs in the immediate posttransplantation period when circulating preformed antibody is deposited diffusely along the endothelium in blood vessels of all sizes. Vascular necrosis occurs because of widespread activation of complement. Concurrent activation of the clotting cascade leads also to extensive thrombosis and secondary coagulation necrosis of the renal parenchyma (15,16).
Only gold members can continue reading. Log In or Register to continue
 Detection of Recipient Pretransplant Alloreactivity
Detection of Recipient Pretransplant Alloreactivity
 Surgical Issues in the Transplant Recipient
Surgical Issues in the Transplant Recipient
 Hematologic Complications of Transplantation
Hematologic Complications of Transplantation
 Non-CMV, Non-hepatitis Viral Infections in the Renal Transplant Patient
Non-CMV, Non-hepatitis Viral Infections in the Renal Transplant Patient
 Medical Complications of the Eyes, Nasopharynx, Dentition, Oropharynx, and Hearing in the Kidney Transplant Recipient
Medical Complications of the Eyes, Nasopharynx, Dentition, Oropharynx, and Hearing in the Kidney Transplant Recipient



