19 Palpable asymptomatic abdominal masses
Case
Mrs PA, a 45-year-old previously well woman presented to her general practitioner for a health check as part of a life insurance renewal. She denied any current illness or symptom, but when her general practitioner carried out an abdominal examination a mass was palpated in the right upper quadrant. The mass was smooth, slightly tender and moved with respiration, suggesting it arose in the liver. Following first principles, her doctor first of all revisited her medical history and noted that Mrs X had been on the oral contraceptive pill for more than 20 years. Furthermore, on close questioning she admitted to intermittent low grade abdominal discomfort in the right upper quadrant over several years, but a little more frequently over the last few months. However, her general practitioner could not identify any other hepatic disease risk factor in her history, such as intravenous drug use or other exposure to hepatitis B or C infection, or exposure to hydatid disease, and could find no other physical abnormality, in particular no evidence of chronic liver disease. Mrs X was referred for liver function tests, viral screens and an abdominal ultrasound scan. Her transaminase levels were mildly elevated, hepatitis B and C serology were negative and there was a solid mass seen on ultrasound scanning. Mrs X was referred to a multidisciplinary hepatology unit and, after more detailed investigation, was eventually found to have a 12-cm mass protruding from the inferior margin of hepatic segment 5. The imaging characteristics including the presence of a central scar were consistent with focal nodular hyperplasia, thought to be unrelated to her oral contraceptive pill consumption. After discussion with a hepatologist, with a hepatic surgeon and with her general practitioner and family, Mrs X elected to undergo surgery for removal of the mass. Subsequent histopathology confirmed the diagnosis of focal nodular hyperplasia. Her recovery was uneventful.
Introduction
Other chapters in this book are orientated to evaluation of symptomatic abdominal masses, abdominal distension and lumps in the groin. Chapter 26 discusses masses detected as incidental findings on abdominal imaging (incidentalomas).
Documenting the Finding of an Abdominal Mass
How was the mass detected, who detected it and when?
Masses within the Abdominal Wall
The different types of abdominal wall hernias and their features are listed in Box 19.1. Abdominal wall hernias are generally easy to characterise as a cough impulse is usually present, the hernia may present in a characteristic position and it may be possible to reduce the hernia. To separate other masses found within the abdominal wall from masses within the abdominal cavity, ask the patient to contract the anterior abdominal muscles by lifting his or her head from the examining couch with hands behind head, or to straight leg raise both legs simultaneously while keeping the head on the bed. This may help to define the mass as follows:
Box 19.1 Causes of abdominal wall masses
Lumps that could occur anywhere on the body
These arise in the skin and subcutaneous fat and include:
Lumps specific to the anterior abdominal wall
Herniae
Retroperitoneal Masses
The retroperitoneal region is subdivided into five regions:
Intraabdominal Masses
Site
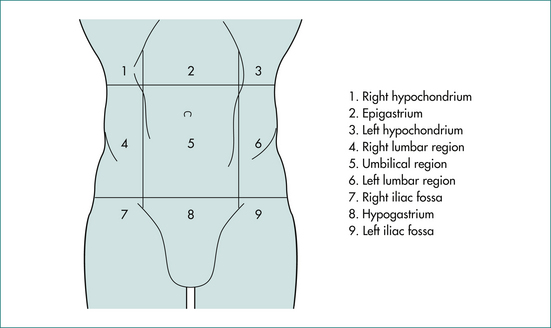
On the basis of position (Fig 19.1), we can start to define the likely organ of origin of an intraabdominal mass as shown in Table 19.1. However, we cannot be certain of the organ of origin of a palpable mass on the basis of its position alone. Organs do not necessarily enlarge concentrically from a fixed point. The pattern of enlargement may be determined by surrounding structures, by retroperitoneal attachments and by the pathological process responsible for the organ enlargement. The liver, for example, is limited by the diaphragm along the superior surface and by the diaphragm and ribs along the lateral surface and so tends to enlarge downwards and inwards. The uterus and bladder are limited by the pelvic walls laterally and below and so tend to enlarge upwards in the midline. The kidneys, aorta and pancreas are retroperitoneal and limited behind by the posterior abdominal wall and so tend to expand from their original site in all directions except posterior. An enlarged segment of small bowel is usually not found in the upper reaches of the abdomen because the transverse mesocolon, the transverse colon and the greater omentum are attached to retroperitoneal tissues along a horizontal line at the level of the inferior border of the pancreas. These three organs tend to form a barrier restricting upward migration of small bowel masses.
Table 19.1 Organ of origin of intraabdominal masses by region
| Right hypochondrium | Epigastrium | Left hypochondrium |
|---|---|---|
| Right lobe of liver | Stomach | Spleen |
| Gall bladder | Left lobe of liver | Pancreas∗ |
| Pancreas∗ | Stomach | |
| Lymph nodes∗ | ||
| Aorta∗ | ||
| Right lumbar region | Periumbilical | Left lumbar |
| Ascending colon∗ | Omentum | Descending colon∗ |
| Right kidney∗ | Transverse colon | Left kidney∗ |
| Aorta∗ | ||
| Retroperitoneal nodes∗ | ||
| Right iliac fossa | Hypogastrium | Left iliac fossa |
| Appendix | Bladder | Sigmoid colon |
| Caecum∗ | Uterus | Iliac aneurysm∗ |
| Iliac aneurysm∗ | Right and left ovary∗ | Left ovary∗ |
| Right ovary | Iliac nodes∗ | |
| Iliac nodes∗ |
∗ Strictly retroperitoneal in position
The likely organ of origin may be defined by the position of the mass as in Table 19.1.
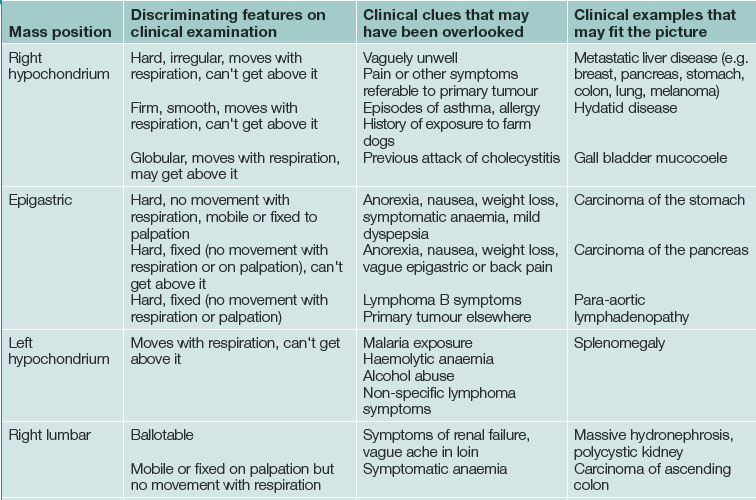
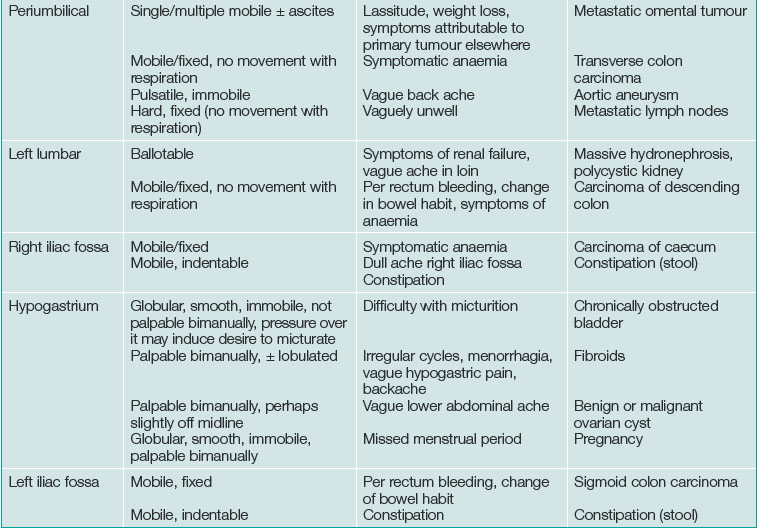
Discriminating clues that may be found on examination and that the patient may report on closer questioning may help establish the causative process. See Table 19.2 and Box 19.2.
Movement with respiration
The diaphragm moves inferiorly with inspiration and back up to its neutral position with expiration. Immediately below the diaphragm are the liver and the spleen. An enlarged liver or spleen will move inferiorly with each inspiratory effort. As well as moving inferiorly, the liver edge and the inferior pole of the spleen move medially relative to the costal margin.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


