1. OVERVIEW OF THE DIGESTIVE SYSTEM
After studying this chapter you should be able to:
1. Understand the key mechanisms of secretion, absorption and motility in the gastrointestinal system.
2. Understand the coordinated and integrated functioning of the digestive system.
3. Understand how function of the digestive system depends on other systems, such as the cardiovascular system.
Introduction: overall function of the digestive system
The cells of the body require adequate amounts of raw materials for their energy requiring and synthetic processes. The raw materials are obtained from the external environment through the ingestion of food. The overall function of the digestive system is to transfer the nutrients in food from the external environment to the internal environment, where they can be distributed to the cells of the body via the circulation. In this chapter, the general principles and basic mechanisms involved in the functioning of the digestive system will be discussed in the context of the system as a whole. The importance of the integration of the digestive system with the other body systems is well illustrated by the problems encountered in non-occlusive ischaemic disease of the gut: a condition in which the defect originates in the vascular system, but serious consequences result from abnormal absorption in the small intestine (see Case 1.1 and Case 1.1).
Case 1.1
An elderly patient, who was being treated with digitalis for congestive heart failure, suddenly developed severe, constant, abdominal pain. The consultant physician examined him and found that he was in circulatory shock, with a low arterial blood pressure, a thready pulse and a sinus tachycardia (rapid heart rate). His abdomen was exquisitely tender to palpitation, with diffuse peritonism (tenderness). The physician suspected from the clinical findings that the patient was suffering from non-occlusive ischaemic disease of the gut. In this condition, the decreased cardiac output results in decreased intestinal perfusion and this, together with other mechanisms, results in the flow of blood to the gastrointestinal tissues being cut off. This disease is often fatal.
Upon consideration of the details of this case, we can ask the following questions:
• What are the main causes of the sudden development of this condition in patients with cardiac failure?
• What are the physiological consequences of reduced flow of blood for the functioning of the small intestine?
• What is the origin of the patient’s pain?
• How are the normal homeostatic mechanisms which control the flow of blood to the gastrointestinal tract perturbed in this condition?
• How can this patient be treated?
Case 1.1
Defect, diagnosis and treatment
Decreased cardiac output results in decreased intestinal perfusion with blood. As the velocity of flow decreases, the viscosity of the blood increases and the blood tends to stagnate in the small vessels. Then microthrombi develop and disseminate in the blood vessels of the mesenteric circulation. There is also a generalized vasoconstriction of the blood vessels that diverts the arterial flow to essential organs. This causes small vessels to collapse. The consequent increase in resistance to flow in the splanchnic circulation, together with the decreased cardiac output and reduced arterial blood pressure results in severely reduced blood flow to the intestines, which eventually become ischaemic.
Reduced blood flow to the gastrointestinal tract results in lack of oxygen and reduced energy substrate supply to the tissues (hypoxia). The result is widespread necrosis of the gastrointestinal mucosa which is most sensitive to hypoxia. This quickly leads to disruption of its functions. The necrosis starts at the tips of the villi that become hypoxic first. It seems probable also that disruption of the brush border of the enterocytes exposes the underlying tissue to the effects of the digestive proteolytic enzymes in the lumen. The intestines become permeable to toxic substances from the contents of the gut lumen, such as bacteria and bacterial toxins, and toxic substances from the necrotic cells. These substances enter the portal circulation. In summary, the barrier function of the gut is lost. There is a profound toxaemia and impairment of the normal body defences, resulting in septic shock. Loss of fluid, electrolytes and blood from the gut will also occur. (This effect mirrors loss in the skin in burns). The loss of the external barrier allows penetration of bacteria into the body as well as fluid loss from it.
The abdominal pain is due to the inflammatory response to ischaemia that accompanies the necrosis. The abdominal tenderness (peritonism) is due to transmural ischaemia of the intestinal wall, which in turn results in secondary inflammation of the parietal peritoneum. Differentiation of this condition from occlusive arterial disease is difficult. Selective angiography, a technique involving the introduction of a radio-opaque substance into the blood, followed by X-radiography, may show narrowed and irregular branches of the superior mesenteric artery, and impaired filling of intramural vessels. In contrast, occlusive disease (such as an embolus) would more often be associated with loss of blood flow to major branches of the mesenteric arteries.
Management of this condition requires measures to maintain the cardiac output, blood pressure, and tissue oxygenation, treatment of infection, and replacement of fluid and electrolytes lost from the gastrointestinal tract. Surgery for heart failure is not safe in the presence of gut infarction. If peritonitis is present, abdominal surgery is required to remove the necrotic intestinal tissue.
Components of the digestive system
Figure 1.1 illustrates the component organs of the gastrointestinal tract, and the associated organs that are essential for the functioning of the digestive system. The gastrointestinal tract consists of the mouth, oesophagus, stomach, small intestine and large intestine. The food is taken into the mouth and moved into the pharynx by the activity of skeletal muscle, then along the rest of the tract by the activity of smooth muscle. The food material is brought to an appropriate semi-fluid consistency, and the nutrients in it are dissolved and degraded by secretions that enter the tract at different locations. These processes are aided by the contractions of the muscles that serve to mix the secretions with the food.
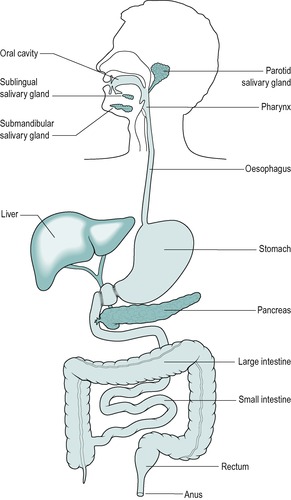
The associated organs situated outside the gastrointestinal tract that are essential for the digestive process are exocrine glands that secrete important digestive juices. These are as follows:
• The three pairs of salivary glands which produce saliva which has a range of functions, but most importantly it provides lubrication of the upper gastrointestinal tract to allow the food to be moved along
• The exocrine pancreas which secretes pancreatic juice which contains most of the important digestive enzymes required to degrade the food into molecules which can be absorbed
• The exocrine liver which produces bile, a secretion which is important for fat digestion and absorption. The bile is also a medium for the excretion of waste metabolites and drugs.
Saliva is released into the mouth. Pancreatic juice and bile enter the duodenum in the upper small intestine (Fig. 1.1). The release of these juices is stimulated when a meal is present in the gastrointestinal tract.
Physiological processes of the digestive system
The physiological processes that are important for the functioning of the digestive system are:
• Digestion
• Absorption
• Motility
• Secretion (and excretion).
Digestion
Digestion is the process whereby large molecules are broken down to smaller ones. Food is ingested as large pieces of matter, containing high molecular weight substances such as protein and starch that are unable to cross the cell membranes of the gut epithelium. Before these complex molecules can be utilized they are degraded to smaller molecules, such as glucose and amino acids.
Absorption
The mixture of ingested material and secretions in the gastrointestinal tract contains water, minerals and vitamins as well as complex nutrients. The products of digestion and other small molecules and ions and water are transported across the epithelial cell membranes, mainly in the small intestine. This is the process of absorption. The transported molecules enter the blood or lymph for circulation to the tissues. This process is central to the digestive system, and the other physiological processes of the gastrointestinal tract subserve it.
Motility
The gastrointestinal tract is a tube of variable diameter, approximately 15 feet long in living human adults. It extends through the body from the mouth to the anus. The food must be moved along it to reach the appropriate sites for mixing, digestion and absorption. Two layers of smooth muscle line the gastrointestinal tract, and contractions of this muscle mix the contents of the lumen and move them through the tract. The process of motility is under the control of nerves and hormones.
Secretion
Exocrine glands secrete enzymes, ions, water, mucins and other substances into the digestive tract. The glands are situated within the gastrointestinal tract, in the walls of the stomach and intestines, or outside it (salivary glands, pancreas, liver, see above). Secretion is under the control of nerves and hormones.
Some substances are excreted, by the liver, into the gastrointestinal tract as components of bile. The gut lumen is continuous with the external environment and its contents are therefore technically outside the body. The faeces eliminated by the intestinal tract are composed mainly of bacteria that have proliferated in the tract, and undigested material such as cellulose, a component of plant cell membranes that cannot be absorbed. Undigested residues are largely material which was never actually inside the body, and is therefore not excreted but eliminated from the body. However, a small portion of the faecal material consists of excreted substances such as the pigments (breakdown products of haemoglobin) that impart the characteristic colour to the faeces.
Quantities of material processed by the gastrointestinal tract
During the course of the day, an adult usually consumes about 800g of food and upto 2litres of water. However, the ingested material is a small part of the material that enters the gastrointestinal tract because secretion into the tract may amount to 7–8L of fluid, the exact amount depending on the frequency and composition of the meals eaten. Figure 1.2 indicates the approximate volumes of fluid entering or leaving the gastrointestinal tract during the average day, and the locations where the processes occur.
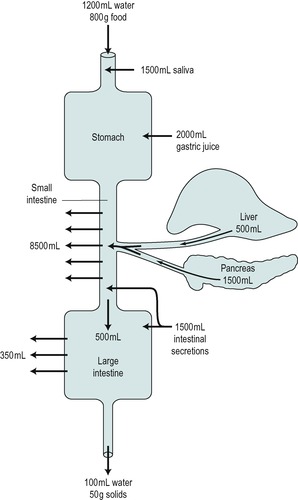
Thus 9–10L of fluid may enter the tract per day. Most of this has been processed when the chyme reaches the large intestine and only 5–10% of it is left to pass on into the colon. Most of this is absorbed in the colon and only approximately 150g is eliminated from the body as faeces. The latter contain about 30–40% solids that are undigested residues and a few excreted substances (see above).
Regulation of ingestion
Intake of food should be adequate to meet the metabolic needs of the individual, but it should not be so much that it causes obesity. Food ingestion is determined by the sensation of hunger. Hunger induces an individual to search for an adequate supply of food. A desire for specific foods is known as appetite. Satiety is the opposite of hunger. It is a sensation that usually results from the ingestion of a meal in a normal individual. The control of hunger can be considered in relation to two categories of sensation:
1. Sensations from the stomach known as hunger contractions or hunger pangs, i.e. ‘alimentary’ regulation concerned with the immediate effects of feeding, on the gastrointestinal tract
2. Subjective sensations associated with low levels of nutrients in the blood, i.e. ‘nutritional’ regulation, concerned with the maintenance of normal stores of fat and glycogen in the body.
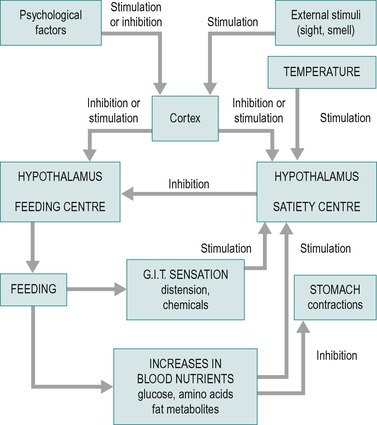
The regulation of food intake is coordinated by neurones in two areas of the brain, known as the feeding (or hunger) centre and the satiety centre. Figure 1.3 indicates some of the factors involved in the regulation of food intake, and the areas of the brain upon which they act. The feeding centre is located in the lateral hypothalamus. Stimulation of neurones in this area causes an animal to eat voraciously (hyperphagia). On the other hand, lesions of this area can cause a lack of desire for food and progressive inanition (loss of weight). In summary, this area excites the emotional drive to search for food. It controls the amount of food eaten and also excites the various centres in the brainstem that control chewing, salivation and swallowing.
 |
| Fig. 1.3 |
The satiety centre is situated in the ventromedial nuclei of the hypothalamus. Stimulation of neurones in this area results in complete satiety, and the animal refuses to eat (aphagia), whereas lesions in this area can cause voracious eating and obesity. The satiety centre operates primarily by inhibiting the feeding centre.
The control of appetite appears to be via higher centres than the hypothalamus, including areas in the amygdala, where sensations of smell have an important role in this control, and cortical areas of the limbic system. These areas are closely coupled to the feeding and satiety centres in the hypothalamus.
Alimentary regulation of feeding
The regulation of feeding by sensation from the alimentary tract is short-term regulation. The feeling of hunger when the stomach is empty is due to stimulation of nerve fibres in the vagus nerve that causes the stomach to contract. These contractions are known as hunger contractions, or hunger ‘pains’. They are triggered by low blood sugar, which stimulates the vagus nerve fibres. However, feelings of hunger or satiety at different times of the day depend to a large extent on habit. Individuals who are in the habit of eating three meals a day at regular times, but miss a meal on an occasion are likely to feel hungry, even if adequate nutritional stores are present in the tissues. The mechanisms responsible for this are not understood.
Other factors are also important in the alimentary control of hunger, such as distension of the stomach or duodenum. This causes inhibition of the feeding centre and reduces the desire for food. It depends mainly on the activation of mechanoreceptors in these areas of the tract, which results in signals being transmitted in sensory fibres in the vagus nerves. The chemical composition of the food in the duodenum is also important. Thus fat in the duodenum stimulates satiety via release of the hormone cholecystokinin (CCK) into the blood, from the walls of the duodenum (see Ch. 5).
Functional activity of the oral cavity, such as taste, salivation, chewing and swallowing is also important in monitoring the amount of food that passes through the mouth. Thus, the degree of hunger is reduced after a certain amount of food has passed through the mouth. However, the inhibition of hunger by this mechanism is short-lived, lasting only 30min or so. The functional significance of this is probably that the individual is stimulated to eat only when the gastrointestinal tract can cope efficiently with food, so that digestion, absorption and metabolism can work at an appropriate pace.
Nutritional regulation of feeding
The regulation of feeding via nutrient levels in the blood serves to help maintain body energy stores. An individual who has been fasting for some time tends to eat more when presented with food, than one who has been eating regular meals. Conversely if an animal is force-fed for some time, it eats very little when the force-feeding ceases but food is made available. The activity of the feeding centre is therefore geared to the nutritional status of the body. The factors that reflect this and control the feeding and satiety centres are the levels of glucose, amino acids and fat metabolites available to them. Glucose is very important in this respect. When blood glucose levels fall, an animal increases its feeding. This returns its blood glucose concentration to normal. Furthermore, an increase in blood glucose concentration increases the electrical activity in neurones in the satiety centre. Neurones in the satiety centre, but not other areas of the hypothalamus, concentrate glucose, and this may be related to its role in the control of hunger. The control of feeding by blood glucose levels is known as the ‘gluco-static’ theory of hunger. To a lesser extent, an increase in the concentration of amino acids in the blood can also reduce feeding, and a decrease enhances feeding.
The extent of feeding in an animal depends on the amount of adipose tissue in the body, indicating a role for fat metabolites in the control of feeding behaviour. If adipose tissue mass is low, feeding is increased. It seems likely that lipid metabolites exert a negative feedback control of feeding. This is known as the ‘lipostatic’ theory of hunger. The nature of the metabolites responsible for this effect is unknown. However, the average concentration of unesterified fatty acid in the blood is approximately proportional to the quantity of adipose tissue fat in the body. Thus, free fatty acids or their metabolites probably also regulate long-term feeding habits, and so enable the individual’s nutritional stores to remain constant.
Obesity can be due to an abnormality of the feeding mechanism, resulting from either psychogenic factors or from an abnormality of the hypothalamic feeding centres. These can be genetic or environmental factors; overeating in childhood is probably one environmental determinant of obesity. Excessive feeding results in increased energy input over energy output. However, this may occur only during the phase when obesity is developing. Once the fat has been deposited the obesity will be maintained by normal food intake. It can only be reduced if energy input is lower than energy output. This can be achieved only by reducing food intake, or by increasing energy output via exercise.
Various drugs have been used in the treatment of obesity. These include amphetamines that increase activity levels and inhibit the feeding centre in the hypothalamus. More recently developed drugs include endocannabinoids that are involved in metabolic homeostasis. These also act by (among other mechanisms) modulation of central nervous system pathways, to suppress hunger via the feeding centre. A promising new drug, orlistat (tetrahydrolipstatin), acts by inhibiting pancreatic lipase, the enzyme that breaks down neutral fat (triacylglycerol) in the small intestine (see Ch. 8). Undegraded triacyl-glycerol is not absorbed in the digestive tract. Although this drug provides an effective treatment for obesity, the absorption of fat-soluble vitamins may also be reduced and the diet should be supplemented with these vitamins to increase the amount absorbed.
Modern treatment of obesity can include surgery to restrict the ability of the stomach to distend, hence providing the sensation of satiety (through suppression of the feeding centre in the hypothalamus), or even, in severe cases, wiring of the jaw to restrict food intake.
Inanition is the opposite of obesity. It can be caused by food deprivation, hypothalamic abnormalities, psychogenic abnormalities or a catabolic state such as that present in advanced cancer. Anorexia nervosa is an abnormal state, believed to be of psychogenic origin, in which the desire for food is lost.
Body temperature is also important in the regulation of feeding. Exposure of an animal to cold causes it to eat more than usual. This has physiological significance because increased food intake increases the metabolic rate, and therefore heat production. It also increases fat deposition for insulation. Exposure to heat in an animal causes it to eat less than normal. These effects involve interaction between centres in the hypothalamus that regulate temperature and the centres that regulate food intake.
Thirst
The sensation of thirst occurs when there is an increase in plasma osmolality, a decrease in blood volume, or a decrease in arterial blood pressure. However, thirst can be satisfied by drinking water before sufficient is absorbed to correct these changes. Receptors located in the mouth, pharynx and upper oesophagus are involved in this rapid response. However, the relief of thirst by this mechanism is short-lived. Complete satisfaction of thirst occurs only when the plasma osmolality, blood volume, and arterial blood pressure are returned to normal. Body fluid hyperosmolality is the most potent of these stimuli. An increase of only 2% can cause thirst. Water intake is regulated by neurones in the hypothalamus in the ‘thirst centre’. Some of these cells are osmoreceptors that are stimulated by an increase in osmolality. The neural pathways involved in the response are not clear, but they may be the same pathways that regulate the release of antidiuretic hormone (ADH, vasopressin), which controls water reabsorption in the kidney tubules. ADH is released from the posterior pituitary in response to changes in osmolality, blood volume and arterial blood pressure (see the companion volume The Endocrine System). Thirst and vasopressin work in concert to maintain the water balance of the body. This axis is disrupted in the hyperglycaemia associated with diabetes mellitus. The raised serum glucose concentration increases the osmolality thereby stimulating thirst. In addition the increase in plasma glucose (which results in excretion of glucose in the urine, causes an osmotic diuresis (excessive production of urine). For this reason patients with new onset diabetes often present with polydipsia and polyuria (see Ch. 9). The resulting hypovolaemia (low blood volume) exacerbates the situation by stimulating thirst even more.
Distribution of blood to the digestive organs
The proper functioning of the digestive system depends on the gastrointestinal tract and associated organs receiving an adequate supply of oxygen and nutrients to meet their metabolic needs. These substances are carried to the tissues by the blood circulation. The blood vessels that supply the digestive organs located in the abdomen (and the spleen) comprise the splanchnic circulation. Over 25% of the output from the left ventricle of the heart can flow through the splanchnic circulation. It is the largest of the regional circulations arising from the aorta. A major function of the splanchnic circulation is to provide fuel to enable the processes of secretion, motility, digestion, absorption, and excretion, to take place. It also functions as a storage site for a large volume of blood that can be mobilized when the need arises. Thus, during exercise, for example, the blood is diverted away from the digestive organs to the skeletal and heart musculature.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


