Chapter 29 Other infections involving the liver
1 Primary bacterial infection of the liver is rare. Systemic infections can cause hepatic derangements, ranging from mild liver biochemical test abnormalities to frank jaundice and, rarely, hepatic failure.
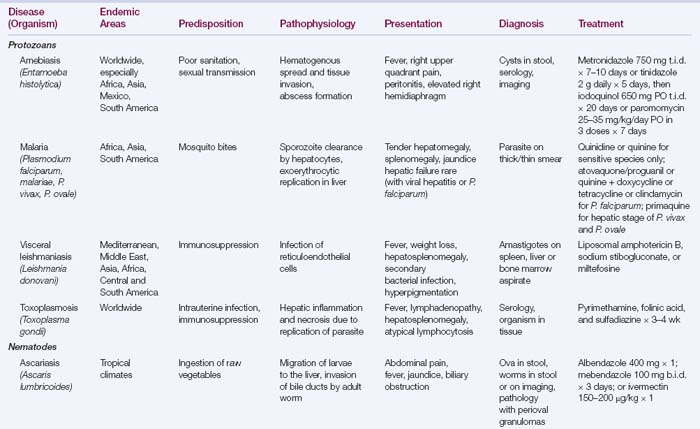
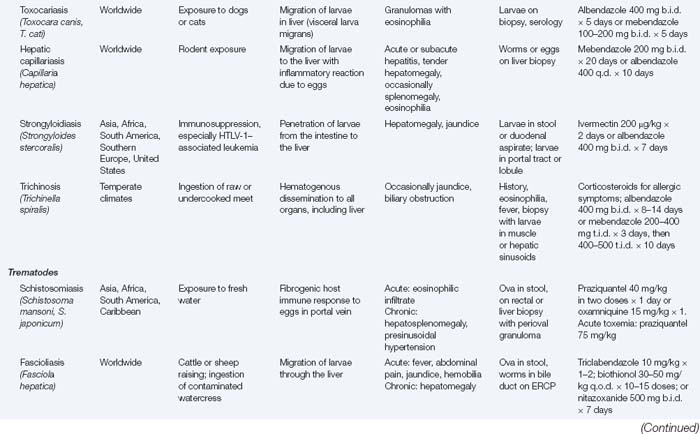
3 Schistosomiasis, capillariasis, toxocariasis, and strongyloidosis evoke strong host inflammatory responses and hepatic fibrosis that contribute to the hepatic manifestations.
4 Leishmaniasis and malaria lead to disease primarily through disruption of reticuloendothelial system function.
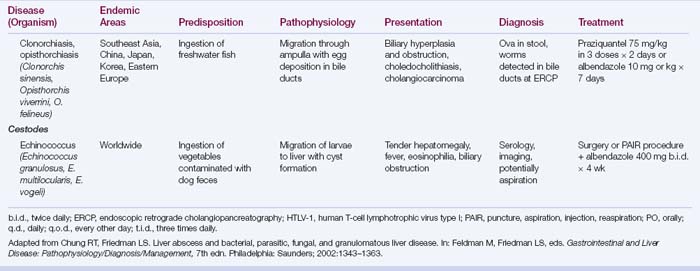
5 Liver flukes and ascariasis cause cholangitis and biliary hyperplasia; liver fluke infection is associated with cholangiocarcinoma.
Bacterial Infections Involving the Liver
Legionella pneumophila
 Pneumonia is the predominant clinical manifestation; abnormal liver biochemical test levels are frequent, usually without jaundice and without affecting the clinical outcome.
Pneumonia is the predominant clinical manifestation; abnormal liver biochemical test levels are frequent, usually without jaundice and without affecting the clinical outcome.

Staphylococcus aureus (toxic shock syndrome)
 This multisystem disease is caused by the staphylococcal toxic shock syndrome toxin (TSST-1) and has a mortality rate of 8%. Originally described in association with tampon use, it is now more frequently a complication of Staphylococcus aureus infections in surgical wounds, mostly in women.
This multisystem disease is caused by the staphylococcal toxic shock syndrome toxin (TSST-1) and has a mortality rate of 8%. Originally described in association with tampon use, it is now more frequently a complication of Staphylococcus aureus infections in surgical wounds, mostly in women. Typical findings include fever, a scarlatiniform rash, mucosal hyperemia, vomiting, diarrhea, and hypotension, with rapid development of multiorgan failure. Hepatic involvement is almost always present, results from hypoperfusion and circulating toxins, and is marked by deep jaundice and high serum aminotransferase levels.
Typical findings include fever, a scarlatiniform rash, mucosal hyperemia, vomiting, diarrhea, and hypotension, with rapid development of multiorgan failure. Hepatic involvement is almost always present, results from hypoperfusion and circulating toxins, and is marked by deep jaundice and high serum aminotransferase levels. Liver histologic findings include microvesicular steatosis, necrosis, and centrilobular cholestasis.
Liver histologic findings include microvesicular steatosis, necrosis, and centrilobular cholestasis.

Clostridium perfringens
 This is usually a mixed anaerobic infection that results in rapid development of local wound pain, abdominal pain, and diarrhea; it is associated with myonecrosis or gas gangrene.
This is usually a mixed anaerobic infection that results in rapid development of local wound pain, abdominal pain, and diarrhea; it is associated with myonecrosis or gas gangrene.


Listeria monocytogenes
 This is characterized by meningoencephalitis and pneumonitis; hepatic involvement in adult human infection is rare.
This is characterized by meningoencephalitis and pneumonitis; hepatic involvement in adult human infection is rare.



Neisseria gonorrhoeae
 Half of all patients with disseminated gonococcal infection have abnormal liver biochemical test levels, mainly elevated serum alkaline phosphatase levels and elevated aspartate aminotransferase (AST) levels. Jaundice is uncommon.
Half of all patients with disseminated gonococcal infection have abnormal liver biochemical test levels, mainly elevated serum alkaline phosphatase levels and elevated aspartate aminotransferase (AST) levels. Jaundice is uncommon.

 This can be distinguished from gonococcal bacteremia by a characteristic friction rub over the liver and negative blood cultures. The diagnosis is made by vaginal cultures for N. gonorrhoeae. Laparoscopy may show characteristic “violin-string” adhesions between the liver capsule and the anterior abdominal wall.
This can be distinguished from gonococcal bacteremia by a characteristic friction rub over the liver and negative blood cultures. The diagnosis is made by vaginal cultures for N. gonorrhoeae. Laparoscopy may show characteristic “violin-string” adhesions between the liver capsule and the anterior abdominal wall.
Burkholderia pseudomallei (melioidosis)
 This soil- and water-borne gram-negative bacterium that causes melioidosis is found predominantly in Southeast Asia and India. The clinical spectrum ranges from asymptomatic infection to fulminant septicemia.
This soil- and water-borne gram-negative bacterium that causes melioidosis is found predominantly in Southeast Asia and India. The clinical spectrum ranges from asymptomatic infection to fulminant septicemia.


Shigella and Salmonella spp.
 Cholestatic hepatitis can be attributable to enteric infection with Shigella species; liver histologic findings include portal and periportal polymorphonuclear infiltration, focal necrosis, and cholestasis.
Cholestatic hepatitis can be attributable to enteric infection with Shigella species; liver histologic findings include portal and periportal polymorphonuclear infiltration, focal necrosis, and cholestasis.



Yersinia enterocolitica
 This infection manifests as ileocolitis in children and terminal ileitis and mesenteric adenitis in adults.
This infection manifests as ileocolitis in children and terminal ileitis and mesenteric adenitis in adults.


Coxiella burnetii (Q fever)
 This is characterized by relapsing fevers, headache, myalgias, malaise, pneumonitis, and culture-negative endocarditis; the liver is commonly affected. The predominant abnormality is an elevated serum alkaline phosphatase level.
This is characterized by relapsing fevers, headache, myalgias, malaise, pneumonitis, and culture-negative endocarditis; the liver is commonly affected. The predominant abnormality is an elevated serum alkaline phosphatase level.


Rickettsia rickettsii (Rocky Mountain spotted fever)
 Mortality caused by this systemic tick-borne illness has decreased considerably as a result of early recognition; a few patients present with multiorgan manifestations and have a high mortality rate.
Mortality caused by this systemic tick-borne illness has decreased considerably as a result of early recognition; a few patients present with multiorgan manifestations and have a high mortality rate.

Actinomyces israelii (actinomycosis)


 Hepatic involvement is present in 15% of cases of abdominal actinomycosis, most often as abscesses, and is thought to result from metastatic spread from other abdominal sites through the portal vein. The course is more indolent than that of other causes of pyogenic hepatic abscess (see Chapter 28). Abscesses may be multiple and in both lobes of the liver.
Hepatic involvement is present in 15% of cases of abdominal actinomycosis, most often as abscesses, and is thought to result from metastatic spread from other abdominal sites through the portal vein. The course is more indolent than that of other causes of pyogenic hepatic abscess (see Chapter 28). Abscesses may be multiple and in both lobes of the liver.











Spirochetal Infections of the Liver
Leptospira spp. (leptospirosis)
1. This is among the most common zoonoses in the world, with a wide range of domestic and wild animal reservoirs. Human-to-human transmission is uncommon. Up to 80% of the population has been exposed in some tropical countries; it is uncommon in the United States. Human disease can occur as one of two syndromes: anicteric leptospirosis and Weil’s disease.
2. Anicteric leptospirosis accounts for more than 90% of cases. It is characterized by a self-limited biphasic course. A few patients have elevated serum aminotransferase and bilirubin levels with hepatomegaly.


3. Weil’s disease is a severe icteric form of leptospirosis and constitutes 5% to 10% of all cases. Complications are mainly the result of direct vascular damage by the Leptospira. The two phases of disease are less distinct:


4. The diagnosis of leptospirosis is made on clinical grounds in conjunction with positive cultures of blood or CSF in the first phase or urine in the second phase. Isolation of the organism is difficult and may require many weeks. Microagglutination testing and serologic testing by enzyme-linked immunosorbent assay (ELISA) may confirm the diagnosis in the second phase.
5. Liver histologic examination reveals individual hepatocyte damage and canalicular cholestasis with mild portal inflammation.
Treponema pallidum (syphilis)



2. Secondary syphilis
 Liver involvement is characteristic (up to 50% of cases) and usually manifests with nonspecific symptoms. Jaundice, hepatomegaly, and right upper quadrant tenderness are less common. Nearly all patients exhibit generalized lymphadenopathy.
Liver involvement is characteristic (up to 50% of cases) and usually manifests with nonspecific symptoms. Jaundice, hepatomegaly, and right upper quadrant tenderness are less common. Nearly all patients exhibit generalized lymphadenopathy.
Liver involvement is characteristic (up to 50% of cases) and usually manifests with nonspecific symptoms. Jaundice, hepatomegaly, and right upper quadrant tenderness are less common. Nearly all patients exhibit generalized lymphadenopathy.






Borrelia burgdorferi (Lyme disease)
 This multisystem disease is caused by the tick-borne spirochete Borrelia burgdorferi. Predominant manifestations are dermatologic, cardiac, neurologic, and musculoskeletal. Hepatic involvement occurs in 20% of affected patients and usually manifests as hepatomegaly with increased serum aminotransferase and lactate dehydrogenase levels.
This multisystem disease is caused by the tick-borne spirochete Borrelia burgdorferi. Predominant manifestations are dermatologic, cardiac, neurologic, and musculoskeletal. Hepatic involvement occurs in 20% of affected patients and usually manifests as hepatomegaly with increased serum aminotransferase and lactate dehydrogenase levels.



Parasitic Diseases that Involve the Liver (Table 29.1)
Protozoal infections
2. Malaria
a. Life cycle (Fig. 29.1)
 The liver is affected during two stages of the malarial life cycle; the pre-erythrocytic phase and the erythrocytic phase, during which symptoms are noted.
The liver is affected during two stages of the malarial life cycle; the pre-erythrocytic phase and the erythrocytic phase, during which symptoms are noted.
The liver is affected during two stages of the malarial life cycle; the pre-erythrocytic phase and the erythrocytic phase, during which symptoms are noted.




