17 Loss of appetite and loss of weight
Case
A 64-year-old man presents with a 3-month history of upper abdominal pain associated with weight loss and mild diarrhoea. He describes the pain as a dull ache and, on specific questioning, says it radiates straight through to the back. The pain is sometimes made worse by eating, and comes and goes. He has lost about 8 kilograms in the last 3 months. He has had, up to three times daily, loose stools which are more smelly than normal, but are not pale and flush away without difficulty. He has lost his appetite. He has not noticed dark urine or pale stools. There is no history of arterial or venous thrombosis or embolism. An upper endoscopy 1 month ago was normal based on the report brought by the patient. He is an ex-smoker, having ceased 10 years ago. He has otherwise been in good health. There is no family history of gastrointestinal disease.
Introduction
Weight loss is defined as a state when the caloric output (from the basal metabolic rate and voluntary activities) exceeds the input. Weight loss that equals or exceeds 5% of body weight (or 4.5 kg) over a 6-month period is arbitrarily defined as clinically significant. Most individuals can sustain a loss of 5–10% of their body weight without any significant health consequences. In a hospital or institutional setting, patients who have lost weight have increased morbidity and mortality, particularly elderly patients and cancer patients. Those who have lost 5 kg or more in the preceding 6 months also have an increased postoperative morbidity and mortality.
Pathophysiology of Anorexia and Weight Loss
Anorexia
Anorexia alone is not a symptom of diagnostic value and can occur in many gut and systemic diseases (Box 17.1). Anorexia should be differentiated from ‘sitophobia’, which is a term used to describe a fear of food because of subsequent abdominal pain. Sitophobia can occur with chronic mesenteric vascular insufficiency (abdominal angina) or small intestinal Crohn’s disease with partial obstruction. Anorexia should also be distinguished from early satiation (a feeling of fullness after eating a small amount such that a normal meal cannot be finished), such as occurs after a partial gastrectomy and in patients whose gastric fundus fails to relax (e.g. after a vagotomy, and in some patients with functional dyspepsia).
Weight loss
Involuntary weight loss is a common manifestation of a variety of disease processes (Table 17.1). Although the precise pathophysiological mechanisms inducing weight loss are unclear, multiple factors have been implicated.
Table 17.1 Selected causes of weight loss
| Cause | Examples |
|---|---|
| Medical conditions | |
| Malignancy | Carcinoma of the pancreas, stomach, oesophagus, colon, liver, lung, breast, kidney |
| Gastrointestinal and liver disease | Malabsorptive states, inflammatory bowel disease, secondary to dysphagia, pancreatitis, hepatitis |
| Cardiovascular disease | End-stage heart failure |
| Respiratory disease | End-stage respiratory failure |
| Renal disease | Chronic kidney disease |
| Endocrine disease | Hyperthyroidism (and hypothyroidism-induced anorexia in elderly patients), hyperparathyroidism, diabetes mellitus, panhypopituitarism, Addison’s disease, phaeochromocytoma |
| Connective tissue disease | Scleroderma, rheumatoid arthritis |
| Infections | HIV, tuberculosis, pyogenic abscess, infective endocarditis, atypical Mycobacterium, systemic fungal infections |
| Neurological disease | Stroke, dementia, Parkinson’s disease |
| Drugs | Amphetamines, cocaine, opiates, serotonin reuptake inhibitors |
| Psychiatric conditions | |
| Depression | |
| Anorexia nervosa | |
| Bulimia nervosa | |
| Alcoholism | |
| Neuroleptic-withdrawal | |
| Miscellaneous conditions | |
| Oral disorders | Ill-fitting dentures, candidiasis, gingivitis |
| Hyperemesis gravidarum | |
Cancer patients may be unable to eat or may not feel like eating (secondary to treatment or depression). Failure to down-regulate energy expenditure in the face of decreased caloric intake can lead to energy imbalance, which may be one of the main mechanisms of weight loss in some cancers. Increased caloric utilisation by tumour tissue may also be a factor, although increases in resting energy expenditure have not been shown to occur in all patients with tumours. In the acquired immune deficiency syndrome (AIDS), poor oral intake, malabsorption, tumour development and repeated infections coupled with a relatively high resting energy expenditure may all have a role. In elderly people, preferential oxidation of fatty acids and an increase in anaerobic glucose metabolism result in inefficient expenditure or wastage of adenosine triphosphate.
Clinical Approach to Anorexia and Weight Loss
The differential diagnosis is extensive (Box 17.1 and Table 17.1), but investigations should be directed by the history and physical examination.
History
Weight loss does not always accompany anorexia. Patients may actually have weight loss with an increase in appetite in malabsorption, hyperthyroidism, uncontrolled diabetes mellitus, phaeochromocytoma or occasionally with lymphoma or leukaemia.
Ask whether the patient is afraid to eat because eating precipitates pain or other gastrointestinal symptoms. Abdominal pain that usually occurs after eating suggests peptic ulcer disease, chronic pancreatitis or chronic mesenteric ischaemia (abdominal angina). Pain after eating may also occur in patients with the irritable bowel syndrome or functional dyspepsia (Chs 6 and 7).
In elderly patients, poor dentition is a common but often overlooked problem. Oral disease resulting from conditions such as vitamin deficiencies, candidiasis or gingivitis can affect mastication. Ask about alterations in taste (dysgeusia), which may make food seem unpalatable. Zinc deficiency may sometimes be responsible for dysgeusia (Ch 3).
Ask about previous medical conditions (e.g. pulmonary tuberculosis, renal disease, previous cancer, cardiac disease) and past surgery. Postgastrectomy syndromes can cause malabsorption (Ch 6). Prior abdominal surgery causes adhesions that can lead to chronic incomplete intestinal obstruction.
Physical examination
Examine for specific features of vitamin and mineral deficiencies (Table 17.2). Glossitis, cheilosis or perioral dermatitis can result from deficiency of vitamins such as riboflavin, pyridoxine or niacin, whereas peripheral neuropathy or ataxia can occur due to lack of thiamine or vitamin B12.
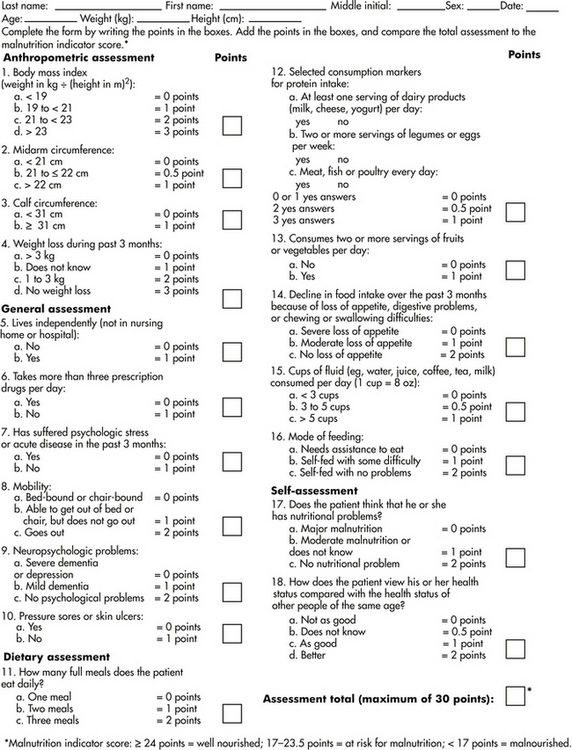
Figure 17.1 Mini nutritional assessment
Reproduced with permission from Guigoz, Y, Vellas, B, Garry, PJ. Assessing the nutritional status of the elderly: The Mini Nutritional Assessment as part of the geriatric evaluation. Nutr Rev 1996; 54(1 Pt 2):S59. Copyright © 1996 International Life Sciences Institute.
Next, conduct a careful gastrointestinal examination. For instance, in a patient with weight loss and jaundice (Ch 23), a pancreatic cancer with biliary obstruction may be the explanation. If stigmata of chronic liver disease are present and abdominal examination reveals a liver mass with or without a bruit, cirrhosis with development of a hepatoma should be considered. Large abdominal masses can occasionally compress the stomach or small bowel, inducing anorexia (Ch 19).
Investigations
The diagnostic work-up needs to be directed towards defining the extent of malnutrition and detecting the underlying cause of weight loss.
Tests to estimate nutritional status
Calculate the BMI (Box 17.2). Other anthropometric measurements include triceps skin-fold thickness and mid-arm muscle circumference to assess the fat reserve and the muscle mass of the body, respectively. These quantitative measurements are useful for follow-up of nutritional status.
Box 17.2 Classification of nutritional status by body mass index (BMI)
| < 16.0 | Severely malnourished |
| 16–16.9 | Moderately malnourished |
| 17–18.4 | Mildly malnourished |
| 18.5–24.9 | Normal |
The prognostic nutritional index predicts the likelihood of developing postoperative complications in patients undergoing gastrointestinal surgery. It is based on a simple linear equation incorporating measurements of serum proteins (albumin and transferrin concentration), subcutaneous fat (triceps skin fold), and immunologic function (delayed skin hypersensitivity).
In the elderly, the mini-nutritional assessment is a valid tool that allows subdivision of patients into nourished, malnourished or at risk of malnutrition (Fig 17.1).
Table 17.2 Clinical findings associated with vitamin and mineral deficiencies
| Findings on physical examination | Associated vitamin deficiencies |
|---|---|
| Mucocutaneous | |
| Dermatitis/cheilosis/glossitis | Riboflavin (B2), pyridoxine (B6), niacin |
| Bleeding/swollen gums | Vitamin C |
| Petechiae/ecchymoses | Vitamins C and K |
| Perifollicular haemorrhages/keratitis | Vitamin C |
| Rash (face/body: pustular, bullous, vesicular, seborrhoeic, acneiform), skin ulcers, alopecia | Zinc |
| Neurological | |
| Peripheral neuropathy | Thiamine/vitamin B12, chromium, vitamin E |
| Dementia/confusion | Thiamine/niacin, zinc, manganese |
| Night blindness | Vitamin A |
| Ophthalmoplegia | Thiamine |
| Haematological | |
| Pallor (anaemia) | Vitamin B12/folic acid, iron, copper |
| Miscellaneous | |
| Dysgeusia | Zinc |
| Fractures | Vitamin D |
| Loosening of teeth, periosteal haemorrhages | Vitamin C |
| Cardiac failure/cardiomyopathy | Thiamine, selenium |
| Hypothyroidism | Iodine |
Tests aimed at detecting the cause
Diagnostic tests can be arbitrarily classified into those of a screening nature and those that target specific abnormalities detected by the history, physical examination or initial screening test results (Table 17.3). The tests are most successful in finding the cause when they are directed by the history and examination findings.
Table 17.3 Investigations for weight loss and examples of diseases to consider
| Diagnostic test | Examples of diseases screened |
|---|---|
| Bedside tests | |
| Urine analysis | Renal cell cancer |
| Laboratory tests | |
| Routine | |
| Full blood count and iron studies | Iron deficiency anaemia from gastrointestinal blood loss |
| Folate/vitamin B12 | Macrocytic anaemia in bacterial overgrowth |
| Electrolytes | Chronic kidney disease, Addison’s disease |
| Liver function tests | |








