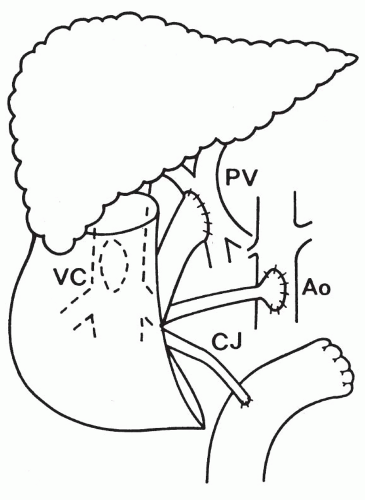
Liver transplantation is an effective and accepted therapy for a variety of chronic, irreversible liver diseases for which no other therapy has proved to be satisfactory. The liver can be transplanted as an extra (auxiliary) organ at another site (
Fig. 58-1) or in the orthotopic location after the removal of the host liver (
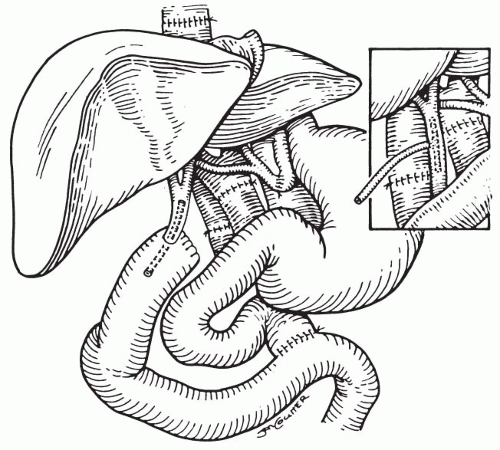
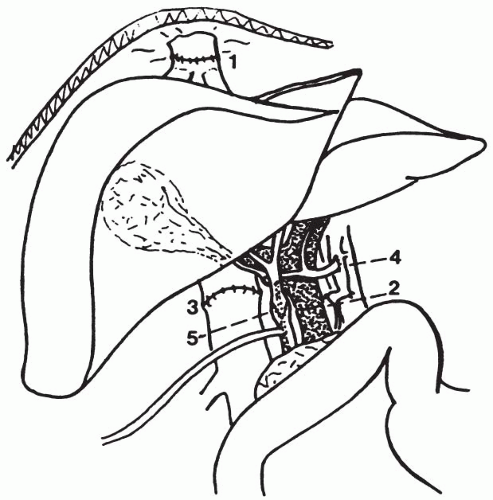
Figs. 58-2 and
58-3). The discussions of this chapter mainly concern the orthotopic liver transplantation (OLT).
Split liver and living-donor liver transplantation has become available and successful. Although the number of patients requiring OLT continues to grow steadily, the number of available donors remains unchanged. Fifteen percent to 20% of patients awaiting liver transplantation die prior to receiving an organ. Currently the majority of patients wait 6 to 24 months for OLT. Although the number of patients requiring OLT continues to grow steadily the number of available organ donors remains unchanged. The referring physician faces three important questions regarding liver transplantation: first, candidacy (patient selection); second, appropriate timing for referral; and third, follow-up care of patients returning from a successful operation.
I. GENERAL INFORMATION.
The American Liver Foundation estimates that in the United States at any one time as many as 5,000 people with end-stage liver disease could benefit from liver transplantation. The two major factors limiting the number of liver transplantations performed are the availability of suitable donor organs and the fact that donor livers are recovered from only about 25% of potential donors. The second factor is due partly to inadequate identification of potential organ donors by physicians. Members of the medical community, especially physicians dealing with patients who may require transplantation (internists, nephrologists, gastroenterologists, cardiologists), must begin to increase their own and their patients’ awareness of the need for donor organs.
In an attempt to increase the number of organ donors, 27 states have passed legislation for required request. This legislation obligates hospitals to have policies in place to offer organ donation as an option to families of patients dying in that hospital. These laws are designed to relieve the attending physician of the burden of requesting organ donation from grieving families by making the request for organ donation part of the routine hospital policy.
Many patients do not receive a liver transplant because they are never referred to a transplantation center. Other patients are referred only after their liver disease has reached its terminal stage, and they often die before a suitable donor organ can be found. To allow all appropriate patients the opportunity to undergo liver transplantation and survive the procedure, physicians must be aware of the criteria for candidacy and for timing of the referral.
There are more than 30 active centers in which liver transplant operations are performed in the United States. For the success of this procedure, centers must maintain high standards and achieve and maintain acceptable 1- and 5-year survival rates. Centers performing fewer than 10 liver transplantations each year are unlikely to maintain the necessary expertise for optimal management of patients with this extremely complex disease. Currently 1-year survival rates range from 80% to 95% and 5-year survival rates are 80% to 85%. The dramatic increase in the survival rates results from the following factors:
A.
Advances in standardization and refinement of the transplantation procedure.
B.
Expertise of anesthesiologists in the prevention and treatment of the metabolic abnormalities that occur in patients with end-stage liver disease during the transplantation procedure.
C.
Use of the venovenous bypass system, which ensures venous return to the heart from both the portal and systemic venous systems during the hepatic phase of the transplantation procedure, reduces blood loss, decreases the incidence of postoperative renal failure, and generally results in less hemodynamic instability during the procedure.
D.
Improved techniques for the identification and support of potential organ donors.
E.
Refinement of operative techniques for the recovery and preservation of the donor livers.
F.
Use of more effective and less toxic immunosuppressive regimens. It is important to remember that successful liver transplantation does not return a patient to normal. Rather, a new disease, a “transplanted liver,” replaces the former disease. However, this new state allows patients a chance for both long-term survival and a more normal lifestyle than were possible during the late stages of their liver disease. After liver transplantation, patients must take immunosuppressive medications for the remainder of their lives. Discontinuation of the prescribed medications may lead to rejection and rapid deterioration in the patient’s condition.
II. CANDIDACY (PATIENT SELECTION).
In the past, patients were referred for liver transplantation only after their disease had reached its end stage. For best results, however, earlier referral to a transplantation center is desirable for all appropriate patients. Because of the variable course of many liver diseases, the determination of the most appropriate time for referral of any patient for transplantation is difficult.
A. Criteria.
There are three general criteria used in most transplantation centers. These are as follows:
1.
The unavailability of other surgical or medical therapies that offer the patient an opportunity for long-term survival.
2.
Absence of complications of chronic liver disease that may significantly increase the patient’s operative risk or lead to the development of absolute or relative contraindications to transplantation.
3.
Understanding by the patient and family of the physical and psychological consequences of the transplantation procedure including the risks, potential benefits, and costs.
B. Indications.
The indications for liver transplantation have been expanding. Currently the indications can best be grouped into four major categories of liver disease:
1.
Chronic irreversible advanced liver disease of any cause
2.
Nonmetastatic hepatic malignancies
3.
Fulminant hepatic failure
4.
Inborn errors of metabolism
Table 58-1 summarizes the indications for liver transplantation used in most transplant centers. More than 60 distinct diseases have been treated with liver transplantation. In adults, the most common diagnoses have been fulminant hepatic failure, chronic active hepatitis, cryptogenic cirrhosis, primary biliary cirrhosis, alcoholic cirrhosis, and inborn errors of metabolism. In pediatric patients, biliary atresia and inborn errors of metabolism are the most common indications (
Table 58-2).
C. OLT for specific disease indications
1. Hepatitis C virus (HCV)-induced cirrhosis
is the most common indication for OLT in adults, accounting for 40% to 60% of OLTs in some centers. The overall 3- to 5-year survival rate after OLT for HCV cirrhosis is 80% to 85%. Prognosis after OLT may be affected by comorbid conditions including renal insufficiency, cryoglobulinemia, and hepatocellular carcinoma (HCC).
There is no effective antiviral regimen to prevent recurrence of HCV in allograft. Fortunately, reinfection rarely (5%-10% of patients) leads to graft failure within the first 3 to 5 years after OLT, but survival rates are lower than in patients with OLT for other causes of cirrhosis in seven or more years after OLT. Cirrhosis occurs in 10% to 30% of patients post-OLT. HCV recurrence in the allograft may be treated by reduction of immunosuppression antiviral therapy or both. Retransplantation for patients with graft failure due to HCV recurrence is controversial and is associated with poor survival (40% 1-year survival).
2. Hepatitis B virus (HBV)-induced cirrhosis
is also a common indication for OLT; however, HBV also recurs in the allograft.
3. Alcoholic cirrhosis/liver disease.
Strict selection of criteria is necessary to identify appropriate patients for OLT. A period of >6 months of sobriety is usually required, but this factor alone is not sufficient for post-OLT recidivism. Many of these patients present with multiple organ systems’ dysfunction and severe malnutrition that requires aggressive preoperative management. Also, other coexistent liver diseases need to be identified (i.e., hemochromatosis, alpha-1-antitrypsin deficiency, viral hepatitis [B, D, C], and ACC). The 5-year survival of patients with alcoholic cirrhosis post-OLT is similar to other patients who undergo OLT for other indications.
4. Liver tumors.
OLT may be indicated for patients with liver tumors who are unable to undergo surgical resection either due to the anatomic location of the tumor or due to the severity of the underlying liver disease (cirrhosis).
Tumors of the liver for which OLT should be considered are HCC, fibrolamellar HCC, epithelioid hemangioendothelioma, hepatoblastoma, and metastatic neuroendocrine tumors.
For HCC, OLT may be offered if the tumor is confined to the liver, documented by imaging (CT or MRI); if the tumor is single (<5 cm) and/or there are fewer than three tumors, each <3 cm in diameter; there is no invasion or thrombosis of the portal vein; and there is no lymph node involvement. For patients fulfilling these criteria, the 5-year survival may approach that of patients who undergo OLT for other causes.
5. Cholestatic liver diseases.
In children, OLT is performed for patients with biliary atresia and Alagille syndrome. In adults, OLT is performed for primary biliary cirrhosis (PBC) and primary sclerotic cholangitis (PSC). A risk score for PBC has been formulated based on patients’ serum bilirubin, albumin, prothrombintre, presence of edema, and variceal bleeding. Patients should be referred for OLT when the lirubin is >10 mg/dL. Posttransplant recurrence of PBC is rare. Patients’ 5-year survival is 80% to 85%.
For PSC, a similar criteria as for PBC has been formulated for OLT and provides more accurate prognostic information. Patients with PSC should be referred for OLT when serum bilirubin is >10 mg/dL. In a small number of patients, PSC may recur in the allograft.