Sexual problems are diffuse in both genders. Although epidemiologic evidence seems to support a role for lifestyle factors in erectile dysfunction, limited data are available suggesting the treatment of underlying risk factors may improve erectile dysfunction. The results are sparse regarding associations between lifestyle factors and female sexual dysfunction, and conclusions regarding influence of healthy behaviors on female sexual dysfunction cannot be made before more studies have been performed. Beyond the specific effects on sexual dysfunctions in men and women, adoption of these measures promotes a healthier life and increased well-being, which may help reduce the burden of sexual dysfunction.
Erectile dysfunction (ED) is defined as the consistent inability to attain or maintain a penile erection of sufficient quality to permit satisfactory sexual intercourse. ED is an important cause of decreased quality of life in men. It has been estimated that the worldwide prevalence of ED will be 322 million cases by the year 2025. The prevalence of this condition increases with age, although ED cannot be defined as necessary consequence of aging. There has been increasing recognition of the many physiologic causes of ED and of the potential for therapy to improve a patient’s quality of life, self-esteem, and ability to maintain intimate relationships. Although epidemiologic evidence seems to support a role for lifestyle factors, limited data are available suggesting that the treatment of underlying risk factors and coexisting illnesses—for example with diet, exercise, and smoking cessation—may improve ED.
The definition of female sexual dysfunction (FSD) includes persistent or recurrent disorders of sexual interest/desire, disorders of subjective and genital arousal, orgasmic disorders, pain, and difficulty with attempted or incomplete intercourse. The debate as to whether FSD should be classified as a dysfunction similar to ED or whether it should be considered a pathologic condition at all is not ended. A study of a US population showed that women reported sexual dysfunction more often than men (43% vs 31%), and 20% women were seeking medical consultation for sexual dysfunction. Moreover, approximately 22% of these women reported feeling distressed by their sexual dysfunction. These percentages have recently been confirmed by the results of Global Study of Sexual Attitudes and Behaviors, an international survey of various aspects of gender and relationships among adults aged 40 to 80 years. Well-designed, random sample, community-based epidemiologic studies, however, are limited and hampered by low response rate, the use of different tools to assess FSD, and the underlying complexity of female sexuality.
Lifestyle factors and sexual function
Healthy behaviors are associated with a reduced risk for ED. In the Health Professionals Follow-Up Study, for example, several modifiable lifestyle factors, including normal weight, increased physical activity, nonsmoking, moderate alcohol consumption, and less television viewing, were associated with maintenance of good erectile function. The results are sparse regarding associations between lifestyle factors and FSD, and conclusions regarding potential influence of healthy behaviors on FSD cannot be made before more studies have been performed.
Overweight and Obesity
Both cross-sectional and prospective epidemiologic studies suggest that overweight and obesity are associated with an increased risk of ED. In particular, the largest population from the Health Professionals Follow-Up Study in the United States, including 31,724 men free of ED at baseline, showed a 40% increased risk of developing ED with obesity. Prospective studies of variable duration from 5 to 25 years of follow-up reported that overweight or obese men had an increased probability (70% to 96% higher) of developing ED compared with normal weight men.
Few studies have investigated the association between obesity and female sexual satisfaction, with nonunivocal results. In a Swedish population studied by Adolfsson and colleagues of 840 younger women (18–49 years) and 426 older women (50–74 years), there was no difference in satisfaction of sexual life between obese and normal weight women, although there was a tendency toward lower sexual satisfaction and sexual desire associated with higher weights in the youngest age group. In 1158 women and men, who were participating in an intensive residential program for weight loss and lifestyle modification or were evaluated for gastric bypass surgery or were obese control subjects not seeking weight loss treatment, approximately 50% of obese women (54.7% to 61.2%) reported difficulty with these aspects of sexual quality of life at least some of the time. The authors and colleagues found a strong negative relationship (r = –0.72) between body weight and sexual function in 52 women with abnormal values of the Female Sexual Function Index (FSFI).
Physical Activity
There is evidence for a protective effect of increased physical activity on ED. In the Health Professionals Follow-Up Study, men in the highest quintile of physical activity were likely to carry a 30% lower risk for ED than those in the referent quintile (sedentary men); in addition, watching television for more than 20 hours per week was also significantly associated with ED (relative risk 1.2) after controlling for leisure physical activity and other health-related factors. A recent meta-analysis of population-based studies demonstrates the existence of a simple dose-response relationship, with higher physical activity conferring lower risks: the adjusted reduction of the risk of having ED was 58% for high activity and 37% for moderate activity compared with men with low physical activity. In a more recent study of 674 men aged 45 to 60 years examined at their place of work, the risk of severe ED was decreased by 82.9% for men with physical activity of at least 3000 kcal per week compared with men under 3000 kcal per week ( P = .018).
There are few studies available that specifically investigated the association between physical activity and FSD. The Boston Area Community Health (BACH) survey was a 2002–2005 community-based epidemiologic study of urologic and gynecologic symptoms, sociodemographics, health status, and psychosocial characteristics in a diverse sample of Boston area residents (N = 3205 women aged 30–79 years). Analyses of sexual problems and their correlates were conducted for the subset of women who engaged in sexual activity with a partner in the previous 4 weeks. A total of 49% of participants were not sexually active, citing lack of interest (51.5%) and lack of a partner (60.8%) as the most common reasons. The likelihood of sexual activity increased with physical activity (odds ratio 1.84, high vs low physical activity level). In a small series of women evaluated prospectively during the natural traverse of menopause, with questionnaires administered at years 1 and year 5, exercise was the only variable associated with sexual satisfaction. In 458 sexually active women participating in the ongoing 5-year longitudinal study, cross-sectional analysis of sexual functioning data revealed that irrespective of stage of menopause, being physically active (at least 30 minutes of physical activity 5 days a week) was associated with higher level of engagement and enjoyment. In 595 women with type 2 diabetes mellitus who completed the FSFI questionnaire, those with higher levels of physical activity were approximately 10% less likely to have FSD compared with those with the lowest level of physical activity.
Smoking
Smoking seems a consolidated risk factor for ED, because it doubles the risk, and passive (secondhand) smoking also increases the risk of ED. Smoking was also correlated with increased ED in the Health Professionals Follow-Up Study, with a 30% increased risk of ED in current smokers compared with nonsmokers. These results have been refined by the publication of a more recent assessment of this population, with a 14-year follow-up period and 3905 new cases of ED from 22,086 participants : smoking was a positive risk factor for ED, both for past smokers (relative risk of 1.1) and current smokers (relative risk 1.4).
There are few studies exploring the relation between smoking and female sexual function. In the Women’s Health Initiative observational study, sexual satisfaction was not associated with smoking in 46,525 respondents answering the sexual satisfaction question. In the BACH survey, smoking history did not modify the probability of having sexual problems. In 595 women with type 2 diabetes mellitus, no association was found between cigarette smoking status and FSD.
Alcohol
Alcohol intake has been associated with decreased ED, probably in part because of the long-term benefits of alcohol on high-density lipoprotein cholesterol and other variables that increase the bioavailability of nitric oxide. In the BACH survey, a multistage stratified random sample was used to recruit 2301 men ages 30 to 79 years from the city of Boston between 2002 and 2005: the results showed a positive, albeit nonsignificant, association with the International Index of Erectile Function (IIEF) score, which was highest with 1 to 3 drinks per day. The data from a population-based cross-sectional study of men’s health to assess the association between usual alcohol consumption and ED in Australia revealed that among current drinkers (n = 1374), the odds were lowest for consumption between 1 and 20 standard drinks per week. On further adjustment for cardiovascular disease (CVD) or for cigarette smoking, age-adjusted odds of ED were reduced by 25% to 30% among alcohol drinkers. In general, the overall findings are suggestive of alcohol consumption of moderate quantity conferring the highest protection.
The studies addressing the relation between alcohol consumption and sexual function in women are scanty. In the 3205 women aged 30 to 79 years participating in the BACH survey, the likelihood of sexual activity increased with alcohol consumption (odds ratio 7.63 ≥3 drinks/day vs none).
Diet and Dietary Habits
Subjects with ED seem to have a vascular mechanism similar to that seen in atherosclerosis and, therefore, a diagnosis of ED may be seen as a sentinel event that should prompt investigation for coronary heart disease (CHD) in asymptomatic men. It seems, therefore, reasonable to assume that dietary factors, which are important in reducing the burden of CHD disease, may also play a role in reducing the occurrence of ED. Physiologic differences in sexual functioning between men and women exist, however, which may relevant to the association between FSD and CHD. In the Women’s Health Initiative observational study, 35,719 respondents women reported satisfaction with sexual activity. There was no increased prevalence or incidence of CVD among sexually active female subjects complaining of dissatisfaction with sexual activity at baseline over 7.8 years of follow-up, and dissatisfaction did not predict incident CVD.
As intriguing this hypothesis is, there are few studies that have assessed the link of diet in ED. The intake of some foods may be less represented in subjects with ED. In a case-control study exploring this relation, the authors compared 100 men who had ED without diabetes and CVD, with 100 age-matched and disease-matched men who did not have ED. In analyses adjusted for the prevalence of associated risk factors, the intake of vegetables, fruits, and nuts and the ratio of monounsaturated lipids to saturated lipids remained the only individual measures associated with ED. In 555 men with type 2 diabetes mellitus attending diabetes clinics located in the area of the Campania County, South Italy, the authors assessed the relation between adherence to Mediterranean diet and sexual function. Median intakes of food groups associated with a Mediterranean diet were calculated, and the participants received a point on the scale if they measured above the median consumption for fish, fruit, legumes, nuts, ratio of monounsaturated to saturated fat, vegetables, and whole grains; otherwise, they received 0 points. Red and processed meat consumption below the median received 1 point, otherwise 0 points. For ethanol, a value of 1 was assigned to men who consumed between 10 and 50 g per day and to women who consumed 5 to 25 g per day. Thus, Mediterranean dietary pattern scores ranged from 0 to 9; higher scores indicated closer adherence to a Mediterranean-type diet. The overall prevalence of ED among diabetic men showed a progressive and significant decline across tertiles: men with the highest score of adherence to the Mediterranean diet had the lowest global prevalence of ED, which remained significant in multivariate analysis that included confounding factors.
The relation between consumption of a Mediterranean-type diet and sexual function has been evaluated in a population of 595 women with type 2 diabetes mellitus, aged 35 to 70 years. Based on the FSFI cutoff score for FSD of 23, women with the highest score of adherence had a lower prevalence of sexual dysfunction compared with women of lower tertiles (47.6%, 53.9%, and 57.8% corresponding to higher, middle, and lower tertiles, respectively; P = .01) ( Fig. 1 ).

Lifestyle Changes and Sexual Function
In general, the validity of the studies can be discussed, because most studies include few participants or short follow-up periods or suffer from selection bias. These studies evaluated the effect of intensive lifestyle changes aimed at reducing body weight and increasing physical activity or investigated the effect of any single component, such as weight loss, increased physical activity, or a particular dietary pattern.
Overall lifestyle changes
Esposito and colleagues looked at the effect of weight loss and increased physical activity on ED in 55 obese men with ED compared with 55 matched-controls, measuring elevated levels of proinflammatory cytokines as a marker of inflammation and endothelial function, and using these markers as an indication of ED. Men assigned to the intervention group were entered in an intensive weight loss program, involving personalized dietary counseling and exercise advice and regular meetings with a nutritionist and personal trainer. The dietary advice was tailored to each man on the basis of food records collected on 3 nonconsecutive days, which had to be done the week before the meeting with a nutritionist. Men in the control group were given general oral and written information about healthy food choices and exercise at baseline and at subsequent bimonthly visits, but no specific individualized programs were offered to them. After 2 years, men randomized to the intervention had lost significantly more weight, increased their physical activity, experienced favorable changes in physiologic measures of endothelial dysfunction, and had significant improvement in their ED score compared with men in the control group. The investigators suggested that the improvement in ED was a potential effect of the endothelial function following the improvement in the inflammatory markers.
Wing and colleagues examined 1-year changes in erectile function in 306 overweight men with type 2 diabetes mellitus participating in the Look AHEAD (Action for Health in Diabetes) trial: in participants assigned to intensive lifestyle intervention (group or individual sessions to reduce weight and increase physical activity), 8% reported a worsening of EF from baseline to 1 year, whereas the percentage in the control participants was 22%. The overall IIEF score improved from 17.3 to 18.6 in the intervention group.
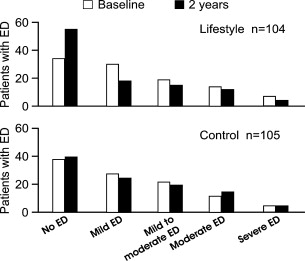
The authors used their database of subjects participating in randomized controlled trials to see whether improvement of erectile function was related to success in achieving lifestyle changes. A total of 209 subjects were randomly assigned to 1 of the 2 treatment groups. The 104 men randomly assigned to the intervention program received detailed advice about how to reduce body weight, improve quality of diet, and increase physical activity. The goals of the intervention were a reduction in weight of 5% or more, a reduction in intake of saturated fat to less than 10% of energy consumed, an increase in intake of monounsaturated fat to 10% or more of energy consumed, an increase in fiber intake to at least 15 g per 1000 kcal, and moderate exercise for at least 30 minutes per day for at least 5 days in a week. The study subjects were ranked according to their success in achieving the goals of the intervention (and given a success score between 0 and 5) at the 2-year examination, with higher scores indicating more goals met: there was a strong correlation between the success score and restoration of erectile function. At the end, men without ED were significantly higher in the intervention group compared with men in the control group ( Fig. 2 ).
Related posts:
 Quercetin for Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Quercetin for Chronic Prostatitis/Chronic Pelvic Pain Syndrome
 The Complex Interplay Between Cholesterol and Prostate Malignancy
Pollen Extract for Chronic Prostatitis—Chronic Pelvic Pain Syndrome
Statin Clinical Trial (REALITY) for Prostate Cancer: an Over 15-Year Wait is Finally Over Thanks to a Dietary Supplement
Heart Health = Urologic Health and Heart Unhealthy = Urologic Unhealthy: Rapid Review of Lifestyle Changes and Dietary Supplements
The Complex Interplay Between Cholesterol and Prostate Malignancy
Pollen Extract for Chronic Prostatitis—Chronic Pelvic Pain Syndrome
Statin Clinical Trial (REALITY) for Prostate Cancer: an Over 15-Year Wait is Finally Over Thanks to a Dietary Supplement
Heart Health = Urologic Health and Heart Unhealthy = Urologic Unhealthy: Rapid Review of Lifestyle Changes and Dietary Supplements
 Prostate Imaging Modalities that Can Be Used for Complementary and Alternative Medicine Clinical Studies
Prostate Imaging Modalities that Can Be Used for Complementary and Alternative Medicine Clinical Studies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


