CHAPTER 22 Left colon resection (medial to lateral approach)
Step 1. Surgical anatomy
♦ The left colon receives arterial input via the inferior mesenteric artery (IMA). Soon after its takeoff from the abdominal aorta, the IMA branches into a left (descending) colic branch and the superior hemorrhoidal artery (SHA). The SHA continues down to the rectum, along the way giving off sigmoidal branches.
♦ The venous drainage of the left colon is into the inferior mesenteric vein (IMV), which passes posterolateral to the IMA, parallel to the aorta in a cephalad direction, to pass under the tail of the pancreas where it joins the splenic vein.
♦ The lymphatic drainage follows the arteries.
♦ The sympathetic plexus interdigitates around the aorta at the base of the IMA, then it coalesces into the left and right hypogastric nerves as they course over the common iliacs and into the pelvis.
♦ The left ureter and gonadal vessels lie in the retroperitoneum posterior to the left colon mesentery.
Step 2. Preoperative considerations
Room setup and patient positioning
♦ Following induction of general endotracheal anesthesia, the patient is placed in a neutral lithotomy position on a well-padded electric operating room table.
♦ Shoulders, hips and knees should be in the same plane. Arms are carefully padded and tucked at the sides using an oversized beanbag or tucked with sheets. Chest straps or tapes may be placed for added security.
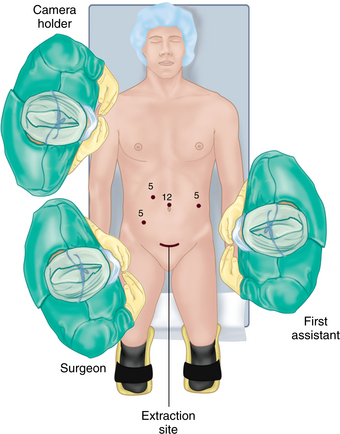
♦ The surgeon and camera operator stand on the patient’s right, assistant on the left (Figure 22-1).
Step 3. Operative steps
Access and port placement
♦ Following port placement, laparoscopic exploration and any necessary adhesiolysis, the patient is placed in a steep Trendelenburg position with the right side tilted down.
Establish plane between the superior hemorrhoidal artery and the sacral promontory:
♦ The small bowel is swept up out of the pelvis and off to the right upper quadrant. The base of the medial (right side of the sigmoid) mesentery over the sacral promontory is exposed by placing the sigmoid mesocolon on anterolateral traction toward the left. The peritoneum over the root of the sigmoid mesentery is scored parallel to and just posterior to the arc of the superior hemorrhoidal artery as it courses over the sacral promontory. This is extended from the sacral hollow up to the root of the IMA (Figure 22-2).
♦ With a gentle blunt anterior to posterior sweeping motion, the areolar, avascular retroperitoneal plane is created. The hypogastric nerves are identified and preserved posteriorly.
♦ Once established, the purplish areolar plane between the sigmoid colon mesentery and the retroperitoneal structures is swept down. This creates a “cave,” which will be deepened up and out to the lateral abdominal sidewall. The left ureter should be identified just lateral to the aorta then coursing down over the left iliac vessels. If it is not visible, the dissection plane may have been too posterior, resulting in the ureter inadvertently being swept anteriorly with the mesosigmoid. If so, the ureter must be identified, freed, then swept posteriorly (Figure 22-3).





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


