Laparoscopic Lateral to Medial
Joseph B. Petelin
Laparoscopic surgery of the right colon may be indicated for a variety of reasons including uncorrectable bleeding localized to the right colon, unresectable masses of the right colon (polyps, submucosal tumors), adenocarcinoma of the right colon, tumors of the appendix or ileocecal region, cecal bascule, volvulus of the right colon, and inflammatory bowel disease of the ileum and ascending colon.
Laparoscopic right colon surgery (LRCS) may be contraindicated in some situations including patient instability precluding general anesthesia, uncorrectable coagulopathy, severe intra-abdominal adhesions, intestinal obstruction with severe distention, and inability of the surgeon to effectively and efficiently perform laparoscopic colonic surgery. The last item is quite probably the most important. It implies that the surgeon should not attempt LRCS unless he or she is able to perform a resection of the disease process (including adequate margins and nodal harvest in cases involving malignancy) in a timely manner.
General patient preparations, as for any general surgery operation, are routine and described elsewhere. Special preparations for right colon surgery usually include mechanical and antibiotic bowel preparation; specific aspects of these preparations are described elsewhere. In some cases, however, these preparations may be altered.
The patient should be informed of (a) the options for the approach laparotomy or laparoscopy and (b) the potential for conversion from a laparoscopic approach to an open approach if deemed appropriate by the surgeon. The author also believes that the patient should be apprised of the surgeon’s training and experience with laparoscopic colectomy. There is a well-documented learning curve (1).
Recent studies suggest that surgeons with little experience and infrequent use of advanced laparoscopic techniques might benefit from a preoperative “warm up” emphasizing laparoscopic instrument handling, suturing, and knot tying.
Positioning: Patient and Personnel
The patient is usually placed in the supine position. He or she must be secured safely to the operating table in order to prevent sliding when the table is rotated or moved from a Trendelenburg to a reverse-Trendelenburg position. A Foley urinary catheter is placed in order to keep the bladder decompressed. Although the author does not routinely use ureteral stents, some surgeons may prefer them, and they certainly may be appropriate for use in appropriately selected settings including large tumors, phlegmons, abscesses, and reoperative surgery.
The surgeon stands on the patient’s left side. If a human camera holder is used, he or she is positioned on the left side. However, if a surgical assistant is used, he or she is preferentially located on the left side as well; although, for spatial considerations the assistant may be required to be located on the right side of the patient. This presents a problem for the assistant because his or her retina is opposite to that of the camera “retina”—a CCD (charge coupled device) or CMOS (complementary metal oxide semiconductor) chip; this scenario is similar to looking into a mirror and results in significant difficulty with accurate instrument manipulations (Fig. 4.1).
Equipment
Standard laparoscopic equipment is obviously necessary for performance of laparoscopic right colectomy. High definition (HD) cameras and monitors enhance the visualization
of the anatomical detail encountered during the laparoscopic portion of the procedure. A straight zero degree scope is used by the author, but many others prefer a 30-degree angled laparoscope.
of the anatomical detail encountered during the laparoscopic portion of the procedure. A straight zero degree scope is used by the author, but many others prefer a 30-degree angled laparoscope.
 Figure 4.1 Patient and personnel positions. |
 Figure 4.2 Room setup with patient and equipment. |
Laparoscopic scissors, clips, staplers, and sutures are commonly used. Over the past decade, a variety of “energy-applying” devices have dramatically improved surgeons’ ability to perform dissection of the mesentery and retroperitoneum. These include unipolar and bipolar radio frequency (RF) coagulating and cutting instruments, and ultrasonic coagulating devices. The wide variety of choices available demands that the surgeon become familiar with his or her selected device(s) prior to starting the operation. The actual setup is illustrated in Figure 4.2.
Because even the antibiotically prepped colon harbors at least some bacteria, it is wise to provide abdominal wall wound protection either by placing the specimen in a plastic bag or covering the wound edges with protective materials prior to removal of the colon from the peritoneal cavity (Fig. 4.3).
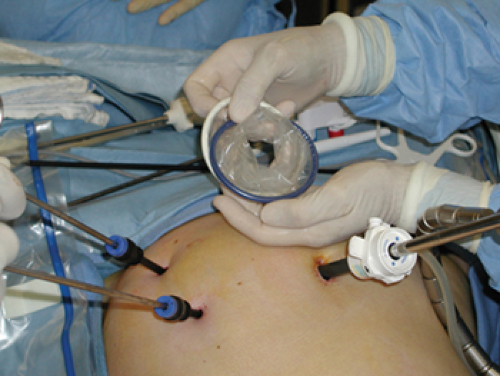 Figure 4.3 Wound protective sleeve. |
Technique
General Comments About the Lateral-to-Medial Approach
Each surgeon has a preference for his or her approach to right colon surgery through a laparotomy approach. Laparoscopy has not changed those preferences, and there are strong proponents for each approach. So, the author believes that a laparoscopic right colectomy can be safely and efficiently performed by either a medial-to-lateral or a lateral-to-medial approach. This treatise is not intended to argue the case for either approach, but rather to describe the concepts and maneuvers involved in the lateral-to-medial approach.
That being said, the author prefers the lateral-to-medial approach because it allows the surgeon to identify one of the most important structures related to laparoscopic right colectomy’the right ureter’early in the case before any potentially difficult and/or dangerous mesenteric dissection is initiated. In his opinion, this method significantly reduces the stress that the surgeon may have while performing the dissection. Instead of worrying about “where is that ureter?” the surgeon can use that “extra brain power” to focus on the most appropriate extent of the dissection. (Consider the alternative wherein the right ureter is not identified early in the medial-to-lateral dissection, and the surgeon is required to continuously use at least “some” computational energy to be concerned about its whereabouts.) The lateral-to-medial approach is also consistent with the so-called “classical” approach to right colectomy used in open surgery by many surgeons. In fact, when laparoscopic right colectomy was first developed it was the preferred method used by most surgeons (2,3,4,5). A decade later reports describing the medial-to-lateral approach surfaced; reasons for this have been debated but this is not the subject of this material (6,7).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


