Parasite
First-line medication(s)
Alternative(s)
Protozoa
Giardia lamblia
Metronidazole or tinidazole
1. Nitazoxanide, albendazole, mebendazole
Entamoeba histolytica
1 Invasive disease
1. Metronidazole or tinidazole
1. Ornidazole and nitazoxanide
2. Asymptomatic carriers, luminal clearance following therapy for invasive disease
2. Paromomycin or iodoquinol
2. Diloxanide furoate
Dientamoeba fragilis
Iodoquinol
Metronidazole, tinidazole, paromomycin
Blastocystis hominis
Metronidazole
Tinidazole, iodoquinol, trimethoprim–sulfamethoxazole
Cryptosporidium
Nitazoxanide
May reduce duration/severity: paromomycin, azithromycin
Cyclospora cayetanensis
Trimethoprim–sulfamethaxazole
Ciprofloxacin
Cystoisospora belli
Trimethoprim–sulfamethaxazole
Ciprofloxacin
Nematodes
Ascaris lumbricoides
Albendazole or mebendazole or levimasole
Ivermectin, nitazoxanide and piperazine citrate
Strongyloides stercoralis
Ivermectin
Albendazole
Hookworms (Necator americanus, Ancylostoma duodenale)
Albendazole or pyrantel pamoate
Mebendazole
Whipworm (Trichuris trichiura)
Mebendazole or albendazole
Ivermectin
Pinworm (Enterobius vermicularis)
Albendazole or mebendazole
Pyrantel pamoate
Cestodes (tapeworms)
Praziquantal
Niclosamide
Diphyllobothrium latum
Praziquantel
Niclosamide
Taenia saginata and Taenia solium
Praziquantel
Niclosamide
Hymenolepis nana
Praziquantel
Niclosamide, nitazoxanide
Entamoeba histolytica
E. histolytica is the most common organism causing pathogenic amoebiasis globally. It was only relatively recently that not one, but three forms of Entamoeba were identified—pathogenic E. histolytica and nonpathogenic E. dispar and E. moshkovski. E. histolytica—although relatively uncommon in the USA, is a common cause of diarrhea in some developing countries, particularly India, Africa, Mexico, and Central and South America. This organism is an uncommon cause of traveler’s diarrhea. It is believed that prevalence is higher among homosexual males, and there have been outbreaks in this population attributed to sexual transmission [9]. Unfortunately, accurate prevalence data likely does not exist because of the recent discovery of nonpathogenic strains that were previously classified as E. histolytica and the large proportion of persons who are asymptomatic carriers [10].
Similar to Giardia, Entamoeba exists in two life forms. There is a more stable cyst form that is responsible for transmission of infection between hosts and a more virulent trophozoite form that is responsible for causing clinical symptoms [5, 11, 12]. Generally, cysts are excreted into soil and are then consumed in contaminated food or water, or via sexual contact. They remain stable in the environment for weeks and are highly virulent—consuming one cyst is adequate to infect a new host. Once consumed, they undergo excystation in the small bowel. The binding and penetration of the trophozoite into the colonic wall result in an invasive colitis. Once the organism has penetrated the colonic mucosa, it is capable of damaging colonic epithelial cells and inflammatory cells through multiple mechanisms [13]. See Figs. 16.1 and 16.2.

Fig. 16.1
Shallow ulcer in the cecum found on screening colonoscopy. The patient had no symptoms. Biopsy showed ameba organisms in the surface of the biopsy. (Pathology pictures courtesy of Dr. Melissa Upton, Seattle, WA)
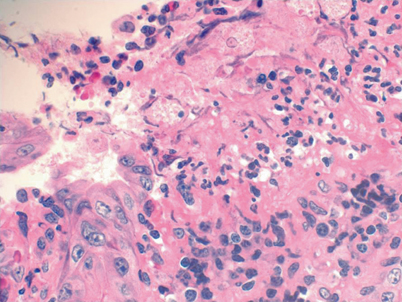
Fig. 16.2
Shallow ulcer in the cecum found on screening colonoscopy. The patient had no symptoms. Biopsy showed ameba organisms in the surface of the biopsy. (Pathology pictures courtesy of Dr. Melissa Upton, Seattle, WA)
The clinical manifestations of E. histolytica are variable. Toxic megacolon, colonic ulcerations leading to perforation or formation of an ameboma—granuloma of the cecum or ascending colon caused by chronic amebic infection—are among the more serious intestinal complications. Fulminant amebic dysentery can ensue and be fatal. However, many patients who test positive for E. histolytica will only have mild diarrhea or be asymptomatic. Liver abscess and other extraintestinal manifestations of E. histolytica are generally seen without recent or concurrent intestinal symptoms [5].
Testing for E. histolytica infection can be achieved with multiple different methods. Conventional stool microscopy, stool antigen testing, and serology with enzyme immunoassay are useful in different clinical settings. Stool microscopy requires laboratory expertise and three separate stool collections on three separate days, making it more tedious. Additionally, microscopy will not differentiate among the three strains of Entamoeba and will only be diagnostic when active intestinal disease is present. Thus, patients suspected of having E. histolytica liver abscess should have serologic testing performed. Stool antigen testing is not universally available, but is efficient and both sensitive and specific for intestinal E. histolytica. Polymerase chain reaction (PCR) is the test of choice to differentiate among strains of Entamoeba. Direct biopsy of the colonic mucosa can be used as a last resort [12].
Treatment is advised in asymptomatic carriers as well as patients with symptomatic disease [13]. Symptomatic patients with suspected invasive disease should be treated initially with systemic therapy for extraluminal disease and then with a luminal therapy for complete clearance. Nitroimidazoles (metronidazole and tinidazole) are commonly used and well tolerated for initial therapy in the setting of invasive disease (invasive colitis, liver abscess). Asymptomatic carriers, and those with invasive disease who have completed initial therapy, should be treated with a luminal agent, most commonly paromomycin or iodoquinol, to prevent both spread to others and development of new or recurrent invasive disease (Table 16.1) [5, 13]. It is important to note that those with peritonitis secondary to colonic perforation will require broad-spectrum antibiotics as well as the two-phase therapy noted above.
Dientamoeba fragilis
Dientamoeba was long considered a commensal organism in the gut, but is now considered pathogenic and should be treated in the absence of other causes for GI symptoms. It has a global distribution and many studies indicate that the global prevalence could be higher than Giardia [14]. The age and gender distribution of patients with Dientamoeba has also been a source of disagreement among various studies [14]. It is clear, however, that this pathogen is most common among populations with other parasitic infections who live in conditions with poor hygiene.
D. fragilis is a binucleate, single-cell organism that is of the trichomonad family but lacks flagella. Transmission is presumed to be fecal-oral, but there is no cyst form of Dientamoeba, so it is less stable in the environment. Because it has been associated with high carriage rates of Enterobius vermicularis (pinworm), some believe helminthic infection may be a vector of transmission [5, 15].
The illness typically causes gas, bloating, abdominal pain, and diarrhea. Diagnosis has improved significantly with the advent of stool PCR testing (sensitivity 96 %), increasing the recognition of this pathogen [15]. Dientamoeba has also been associated with chronic bowel symptoms, such as IBS, and thus, if found in patients who have chronic symptoms of unclear etiology, treatment is suggested [14]. Providers should consider testing for pinworm infection in patients who test positive for D. fragilis. Interestingly, despite the lack of invasiveness of this organism, it is associated with eosinophilia, perhaps because of concurrent pinworm infection. Treatment is with a nitroimidazole (i.e., metronidazole) and several regimens have been studied and found effective (Table 16.1).
Blastocystis Species (Blastocystis hominis)
Blastocystis species (previously referred to as B. hominis) are similar to D. fragilis in that their role as pathogens is still emerging. They have a global distribution and can affect both children and adults. Zoonotic transmission and fecal–oral routes of infection have been implicated. Thus, it is not surprising that higher rates of infection have been observed in developing countries where infection rates from 30 to 50 % have been observed, compared to only 5–10 % in developed countries. Immunocompromised hosts (HIV, transplant recipients) are also more commonly affected [16].
Blastocystis species are anaerobic organisms that have been observed to have four major life forms and significant genetic diversity, which led to their renaming from B. hominis to B. species. Once they have been ingested, they live in the cecum and colon of their hosts. While asymptomatic infection can occur, symptoms can include diarrhea, flatulence, bloating, abdominal pain, nausea, and anorexia. Additionally, there is some association with urticarial disease [16]. Diagnosis is challenging and most frequently made with stool microscopy; however, enzyme-linked immunosorbent assay (ELISA) and PCR tests are likely superior. Treatment requires some clinician judgment because infections can be self-limited or asymptomatic and may not require therapy. Metronidazole and trimethoprim–sulfamethoxazole (TMP-SMX) are two commonly prescribed medications that are effective for treating Blastocystis species [5, 16].
Coccidia
Cryptosporidium
Cryptosporidium is a common enteric pathogen that was identified in the 1970s and has been known to cause prolonged and severe diarrhea as well as biliary disease. Both children and adults are affected by this pathogen, but prevalence is higher among children [17]. In fact, it appears to be one of the most common causes of moderate to severe diarrheal illness among children in Africa and Asia [17] .
Cryptosporidia are a group of intracellular protozoa with approximately 20 species and multiple genotypes. C. parvum and C. hominis are the main species causing human disease [18]. Transmission is by consumption of environmentally stable oocysts, which then undergo excystation in the small bowel leading to infection of enterocytes, where reproduction occurs. Infection can also extend into the biliary tract in immunocompromised hosts.
Outbreaks are primarily associated with water contaminated by animal or human feces. Prevention of transmission requires heating or freezing water, as chlorination is ineffective in killing the stable oocysts [18]. Because of its environmental stability, fecal–oral transmission is possible by multiple modalities. There have been outbreaks in children in US daycare centers. Prevalence may also be higher when there is close contact with animals such as in rural areas .
The spectrum of clinical illness is broad, ranging from self-limited (10–14 day duration) mild diarrheal illness in immunocompetent patients to a chronic enteritis with documented destruction of intestinal villi and occasionally biliary tract involvement in HIV positive or otherwise immunocompromised patients [19]. In the later situations, patients can become severely malnourished and dehydrated. Up to one third of these patients can have biliary tree involvement with inflammatory strictures, acalculous cholecystitis, and pancreatitis [20, 21].
Diagnosis of cryptosporidiosis is generally made with stool microscopy, which can identify spores. It is necessary to request specific acid fast stains to identify cryptosporidium because a standard ova and parasite stool evaluation may not be diagnostic. More modern methods of detection include ELISA antibody assays, but these are costly and not widely available. Additionally, tissue biopsies may reveal the organism on hematoxylin and eosin staining.
Treatment is usually only necessary in immunocompromised patients with severe and unremitting illness. Unfortunately, the efficacy of currently available treatments is not consistent and still under investigation [5]. In patients with immune suppression due to HIV infection, treatment of the HIV with highly active antiretroviral therapy (HAART) to increase CD4 count can lead to clearance of the parasite [20, 21]. Supportive care is essential and antimicrobial agents are aimed at reducing disease severity and duration. The Centers for Disease Control and Prevention (CDC) supports treatment with nitazoxanide, which is Food and Drug Administration (FDA) approved for children over 1 year of age. A randomized controlled trial demonstrated efficacy for HIV negative children, but not HIV positive children [22] .
Cyclospora cayetanensis
Cyclospora is an obligate intracellular protozoan that causes enteritis. It was identified in the 1980s and initial cases were confused with cryptosporidium. The infections are similar in that Cyclospora also causes more severe and protracted disease among immunocompromised hosts (HIV and transplant patients). Additionally, in non-endemic areas, patients typically experience more severe symptoms and in endemic areas, symptoms tend to decrease with age and be most severe in younger children, implying an acquired tolerance [23].
Symptoms are also similar to cryptosporidium, with watery diarrhea, nausea , anorexia, fatigue, weight loss, low-grade fever, and occasionally biliary tract involvement. The diarrheal illness can be prolonged beyond 3 weeks, even in immunocompetent patients.
Transmission is not person to person because oocysts require time (7–15 days) to become infective after shedding [23]. Outbreaks have been traced to contaminated water supplies and large food outbreaks—raspberries imported from Guatemala in 1996 and cilantro and salad mix from Mexico in 2013 [24, 25].
Diagnosis is via stool microscopy, but is improved with acid-fast stains and will not typically be seen on standard ova and parasite testing. Treatment with TMP-SMX is first line. Ciprofloxacin can be used in case of sulfa allergy, but is less effective [23].
Cystoisospora belli (Isospora belli)
This is the least common of the three coccidia known to infect humans. It is an obligate intracellular protozoan that infects the small bowel and colon. It is endemic in tropical and sub-tropical areas, but there have been rare case reports of outbreaks in non-endemic locations in daycare and institutional settings [26]. The populations typically affected by this organism are immunocompromised patients and travelers. Transmission appears to be similar to the other coccidia and likely not via person to person transmission, but rather through contaminated water and food.
Like the other coccidia , the symptoms include watery diarrhea, flatulence, anorexia, headache, vomiting, and malaise. Cystoisospora is associated with reports of reactive arthritis and rarely biliary complications such as acalculous cholecystitis [27].
Diagnosis is typically made on stool microscopy and, like the other coccidia, requires acid-fast staining and laboratory expertise. Stool PCR testing methods are becoming more available. In rare circumstances, duodenal aspirates have also been used.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


