Chapter 12 Hepatorenal syndrome
Overview
1. The term hepatorenal syndrome (HRS) was initially applied to many different disorders involving the liver and the kidney.
2. During the 1960s and the 1970s, nephrologists in the United States popularized the term to define renal failure in cirrhosis.
TABLE 12.1 Diagnostic criteria for hepatorenal syndrome
| 1. Cirrhosis with ascites |
| 2. Serum creatinine level greater than 133 μmol/L (1.5 mg/dL) |
| 3. Lack of improvement in serum creatinine level (i.e., lack of a decrease to a level of ≤ 133 μmol/L) after ≥2 days following diuretic withdrawal and volume expansion with albumin; recommended dose of albumin: 1 g/kg of body weight per day up to a maximum of 100 g/day |
| 4. Absence of shock |
| 5. Lack of current or recent treatment with nephrotoxic drugs |
| 6. Absence of parenchymal kidney disease as indicated by proteinuria >500 mg/day, microhematuria (>50 red blood cells/high-power field), and/or abnormal renal ultrasonography |
Definition
1. Renal failure, estimated by a level of serum creatinine greater than 1.5 mg/dL, occurring in a patient with advanced liver disease and portal hypertension



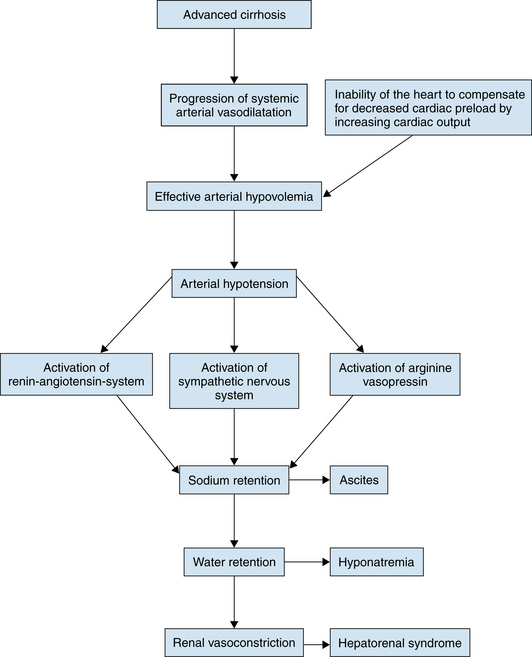
Pathogenesis



3. Systemic hemodynamics
 Hemodynamic alteration results from severe arterial vasodilation located mainly in the splanchnic territory.
Hemodynamic alteration results from severe arterial vasodilation located mainly in the splanchnic territory.
 In the setting of increased activity of vasoconstrictor systems, marked renal vasoconstriction develops.
In the setting of increased activity of vasoconstrictor systems, marked renal vasoconstriction develops.
Hemodynamic alteration results from severe arterial vasodilation located mainly in the splanchnic territory. In the setting of increased activity of vasoconstrictor systems, marked renal vasoconstriction develops.
In the setting of increased activity of vasoconstrictor systems, marked renal vasoconstriction develops.

4. Vasoconstrictor systems










5. Vasodilatory factors





b. Nitric oxide (NO)
 Inhibition of both NO and PGs induces renal vasoconstriction in patients with cirrhosis and ascites.
Inhibition of both NO and PGs induces renal vasoconstriction in patients with cirrhosis and ascites.


 Inhibition of both NO and PGs induces renal vasoconstriction in patients with cirrhosis and ascites.
Inhibition of both NO and PGs induces renal vasoconstriction in patients with cirrhosis and ascites.