Chapter 3 HEARTBURN, ACID REGURGITATION AND BARRETT’S OESOPHAGUS
DEFINITIONS AND SPECTRUM
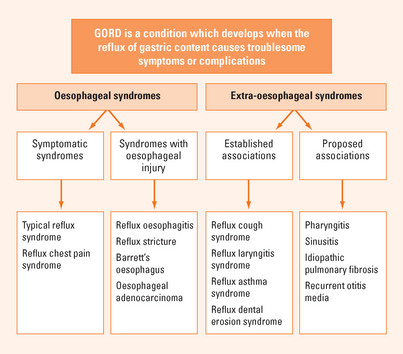
Heartburn is defined as a burning sensation in the retrosternal area and regurgitation as the perception of flow of refluxed gastric content into the mouth or hypopharynx. These are the cardinal symptoms of gastro-oesophageal reflux. Reflux is a physiological event but excessive reflux exposes the patient to the risk of physical complications or symptoms that impair quality of life. Gastro-oesophageal reflux disease (GORD) is defined as a condition which develops when the reflux of stomach contents causes troublesome symptoms or complications. Thus, in the absence of physical complications the definition depends on the impact of symptoms on an individual. Frequently, significant impairment of well-being (quality of life) occurs when symptoms occur on two or more days a week. GORD can be divided into oesophageal syndromes and extra-oesophageal syndromes (Figure 3.1). The former includes symptomatic syndromes of typical reflux symptoms and reflux induced chest pain and syndromes associated with oesophageal injury including oesophagitis (erosive GORD), strictures, Barrett’s oesophagus and the small risk of oesophageal adenocarcinoma. Extra-oesophageal reflux syndromes include the established associations with cough, laryngitis and asthma as well as other putative associations.
EPIDEMIOLOGY, RISK FACTORS AND NATURAL HISTORY
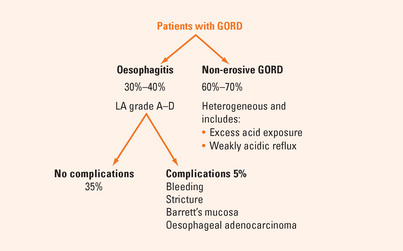
Most patients with GORD have normal oesophageal mucosa at endoscopy (Figure 3.2). Only about one-third of patients with reflux disease have reflux oesophagitis confirmed by endoscopically visible mucosal breaks (erosions or ulceration).
PATHOPHYSIOLOGY
Hiatal hernia is common in reflux disease. Hiatal hernia increases the likelihood that reflux will occur by impairing LOS function. However, the presence of a hiatal hernia does not necessarily mean that reflux disease is present.
DIAGNOSIS
Symptom recognition and assessment
Atypical symptoms include chest pain, which may mimic cardiac pain, and symptoms associated with extra-oesophageal manifestations of GORD including cough, sore throat, hoarseness and wheeze. GORD should be considered in patients who present with no other apparent cause for these symptoms although most patients with reflux-induced extra-oesophageal symptoms will also have typical GORD symptoms.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


