CHAPTER 20 Hand-assisted right colectomy
Step 1. Surgical anatomy
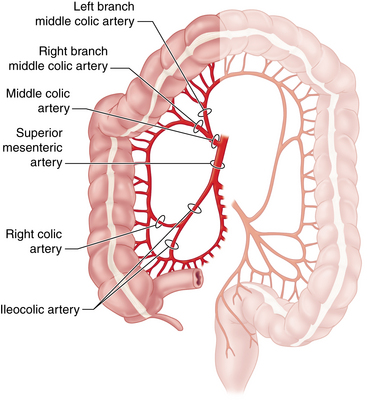
♦ Familiarity with the vascular anatomy of the right colon is essential to the safe conduct of a minimally invasive right colectomy (Figure 20-1). Vascular anatomy also significantly determines resection of colonic malignancies. Several key points guide the laparoscopic surgeon:





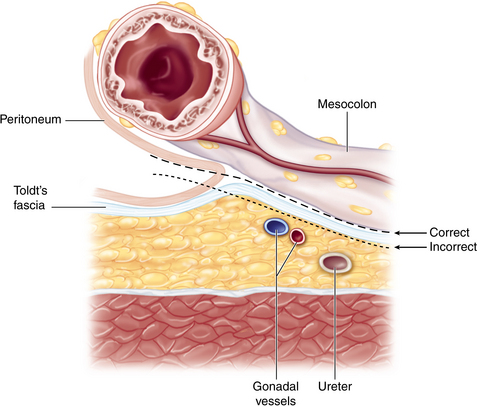
♦ The embryologic fusion plane originates laterally at the white line of Toldt, which occurs where the parietal peritoneum fuses with the visceral peritoneal reflection around the colon and its lateral extension (Figure 20-2). The correct dissection plane is the bloodless embryologic fusion plane. When properly mobilized in this plane, the colon reflects medially on its mesentery to become a nearly midline structure. When the dissection is carried posteriorly past the white line of Toldt, violating the parietal peritoneum as it extends across the retroperitoneal structures, the ureter and gonadal vessels are put at risk and mobilization of the colon is limited.
♦ Awareness of the relationships between the cecum, ascending colon, hepatic flexure, and proximal transverse colon to neighboring structures helps to maintain orientation during surgery and prevents injury:
 The duodenal sweep can be appreciated medial and caudal to the hepatic flexure mesocolon. Risk of injury to the portal triad can be averted by avoiding performance of a Kocher maneuver.
The duodenal sweep can be appreciated medial and caudal to the hepatic flexure mesocolon. Risk of injury to the portal triad can be averted by avoiding performance of a Kocher maneuver.



♦ Surface anatomy considerations principally help with optimal port placement:
 Preoperative knowledge of a redundant transverse colon would suggest more caudal placement of the periumbilical hand port incision.
Preoperative knowledge of a redundant transverse colon would suggest more caudal placement of the periumbilical hand port incision.
Step 2. Preoperative considerations
Patient preparation
♦ Given that the majority of right colectomies are performed for neoplastic diseases (cancer or endoscopically unresectable polyps), staging must be complete before going to the operating room:
 A computed tomography (CT) scan of the chest, abdomen, and pelvis is central to the metastatic workup. A positron emission tomography (PET) scan is sometimes also necessary.
A computed tomography (CT) scan of the chest, abdomen, and pelvis is central to the metastatic workup. A positron emission tomography (PET) scan is sometimes also necessary.
♦ Lesions must be appropriately localized preoperatively. Although all of the patient’s physicians are concerned about making the correct diagnosis, only the surgeon has to perform a resection and must manage the technical details of this procedure:
 Review the colonoscopy report; note the expected location of the target lesion and the presence and character (including pathology report) of any other lesions.
Review the colonoscopy report; note the expected location of the target lesion and the presence and character (including pathology report) of any other lesions.


♦ Plan the extent of resection with regard to both margins and vascular ligation:
 The right branch of the MCA should be included for resection of neoplasms of the cecum or the proximal ascending colon.
The right branch of the MCA should be included for resection of neoplasms of the cecum or the proximal ascending colon.

♦ Past surgical history and an abdominal examination may reveal risks that could present challenges to a minimally invasive approach:
 Surgical scars and history of adhesions or bowel obstruction may alter port site placement or technique of entry.
Surgical scars and history of adhesions or bowel obstruction may alter port site placement or technique of entry.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


