Fig. 10.1
The 6-cm incision provides excellent exposure of small bowel for neobladder reconstruction
Once the neobladder is complete, we estimate the most dependent portion where we think the urethra will be anastomosed. We place a dyed 0 Vicryl™ figure-of-eight suture at the estimated 6-o’clock portion of the neourethra that will be used as a handle by the console surgeon’s fourth arm using a ProGrasp™ forceps (Fig. 10.2). An additional suture is placed in the same position and sutured to the red Robinson catheter that is in the urethra. This acts as an additional handle for the bedside assistant to help bring the neobladder down into the pelvis. An undyed Vicryl™ is placed at the 12-o’clock portion of the neourethra to give the console surgeon better orientation of the pouch and to provide an additional handle with which to manipulate the pouch.
Fig. 10.2
The neobladder is completed with the 6 and 12-o’clock sutures placed at the site of the anticipated neourethra
The neobladder is then placed into the pelvis with only the afferent limb and bilateral ureters exposed at the midline incision (Fig. 10.3). A medium-sized Alexis® Wound Protector/Retractor (Applied Medical, Rancho Santa Margarita, CA) is used to improve exposure for the uretero–ileal anastomoses.
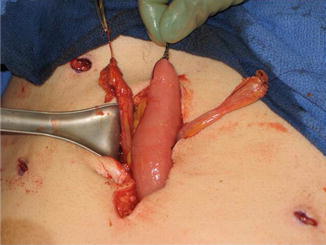
Fig. 10.3
The completed neobladder is placed back into the abdomen, leaving only the ureters and afferent limb exposed for the uretero–ileal anastomoses
The ureters are once again reinspected to ensure they are oriented in their correct anatomic positions. Each ureter is then spatulated and individually sewn in a Bricker end-to-side fashion with interrupted 4-0 Vicryl™ sutures. Each uretero–ileal anastomosis is stented with an 8Fr feeding tube that is brought out through an opening in the afferent limb and beside the right paramedian robotic port. The feeding tubes are secured at the afferent limb with a 3-0 plain gut purse string suture.
The midline incision is then closed to the level of the camera port site. We utilize four preplaced interrupted size 1 polypropylene sutures at the superior aspect of the incision where the camera port is replaced. We are then able to tie down one or two of the interrupted sutures with the port in place to ensure an airtight seal for re-insufflation. The use of an AirSeal® Access Port (Surgiquest, Milford, CT) also helps facilitate adequate insufflation after re-docking. The robot is then re-docked.
Steps Performed After Re-docking the Robot
The urethral anastomosis is performed robotically using either a 0 or 30° down lens. We first inspect the uretero–ileal anastomoses to ensure they are lying in their correct orientation.
The redundant sigmoid colon is moved out of the pelvis. The neobladder is then brought down into the pelvis by the console surgeon using the preplaced 6-o’clock Vicryl™ handle and the fourth arm. The assistant can aid in the maneuver by placing gentle traction on the red Robinson catheter that is also attached to the 6-o’clock position of the neobladder.
Occasionally, the neobladder does not completely reach the urethra, creating tension at the anastomosis. Two maneuvers can be employed to decrease this tension. The first is simply perineal pressure. The second is to undock the robot, minimize the Trendelenburg, and re-dock the robot.
The site of the urethral anastomosis on the neobladder is opened using a robotic shear. This site is determined by choosing an area where the opening is well visualized and easy to work with.
Using the 2-0 Vicryl™ suture that was preplaced at the 6-o’clock position of the urethra at the time of the urethral division, we begin the urethral anastomosis by re-approximating the urethral plate with a simple interrupted suture. The anastomosis is then continued and completed by running two interlocked 3-0 V-Loc™180 6 in. sutures bilaterally to meet at the 12 o’clock position where the sutures are tied. Special attention is given to cinching down on the V-Loc™ suture after each complete pass through the urethra and neobladder in order to ensure a watertight anastomosis.
The completed anastomosis is tested by irrigating the neobladder with 60–120 ml of normal saline. Any visible area of extravasation from either the neobladder or the anastomosis is reinforced with an additional 3-0 Vicryl™ suture. A new two-way 18F hematuria catheter is placed into the neobladder to gravity drainage.
A closed suction drain is placed through the left paramedian robotic port and placed over the urethral anastomosis and adjacent to our uretero–ileal anastomoses. The drain and stents are secured with sutures. The robot is then undocked. The closure of the midline incision is completed with the preplaced polypropylene sutures. The stents are cut 5 cm from the skin and placed to gravity drainage using a urostomy drainage bag, and the skin incisions are closed.
Indiana Pouch Continent Cutaneous Catheterizable Reservoir
With the Indiana pouch, minimal steps are required prior to undocking the robot. As with the neobladder, the ureteral sutures are secured with a laparoscopic grasper through the right iliac port.
We undock the robot but keep the abdo-men insufflated with all ports in place. The Trendelenburg is decreased and the table tilted left as far as possible. Using our existing port placements, we use a conventional laparoscopic technique to mobilize the right colon and hepatic flexure.
The table is then leveled, the ports are removed, the midline camera incision is extended inferiorly 7–8 cm, and the specimen is removed. This incision is larger than the incision made for the neobladder because the pouch tends to be bigger and this also allows us better exposure for the uretero–colonic anastomoses. In obese patients, the size of this incision may need to be further increased to optimize exposure.
We isolate the 15 cm of proximal ileum along with 31 cm of right colon (Fig. 10.4). The avascular plane of Treves is divided to allow mobility to our stomal segment. Bowel continuity is then reestablished using a side-to-side ileal–colic stapled bowel anastomosis. The mesenteric trap is then closed.
 History of Minimally Invasive Techniques for Radical Cystectomy with Urinary Diversion
Robot-Assisted Radical Cystectomy: Male
Perioperative Care: The Radical Cystectomy Pathway
Perioperative Outcomes and Complications of Robot-Assisted Cystectomy
History of Minimally Invasive Techniques for Radical Cystectomy with Urinary Diversion
Robot-Assisted Radical Cystectomy: Male
Perioperative Care: The Radical Cystectomy Pathway
Perioperative Outcomes and Complications of Robot-Assisted Cystectomy
 Cost of Robot-Assisted Radical Cystectomy
Cost of Robot-Assisted Radical Cystectomy
 Robot-Assisted Intracorporeal Ileal Conduit
Robot-Assisted Intracorporeal Ileal Conduit




Related posts:
History of Minimally Invasive Techniques for Radical Cystectomy with Urinary Diversion
Robot-Assisted Radical Cystectomy: Male
Perioperative Care: The Radical Cystectomy Pathway
Perioperative Outcomes and Complications of Robot-Assisted Cystectomy
Cost of Robot-Assisted Radical Cystectomy
Robot-Assisted Intracorporeal Ileal Conduit
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
