Computed tomographic colonography (CTC) is a major advance in colon cancer diagnosis and screening, and will likely join mammography as a first-line imaging modality in the prevention of cancer. Cancer screening has the potential benefits of early discovery of curable lesions and early treatment of the diseases being screened for. However, it may also have the unexpected result of leading to the discovery of incidental findings. This may result in further diagnostic evaluation or intervention with the possibility for increased patient morbidity and health care costs.
ADVANTAGES
The ability of CTC to identify extracolonic lesions is often viewed as advantageous particularly by patients who are increasingly becoming advocates for their own health care (see
Table 8.1). Unlike all of the other colon cancer screening tests, CTC (and magnetic resonance colonography) has the ability to directly detect lesions outside of the colon that may be completely incidental or may account for the patients presenting symptoms for CTC.
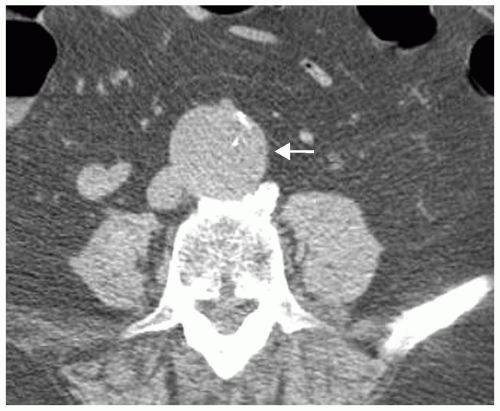
Abdominal aortic aneurysms (AAA) are often identified as completely incidental findings on CTC and those that are large enough (≥5 cm) will require surgical or endovascular repair (see
Figure 8.1). In a study of 243 patients undergoing elective repair of abdominal aortic aneurysm, 62% of cases were discovered incidentally.
1 The impact on future risk to the patient is significant. The mortality rate associated with AAA is much lower for elective surgery (5%) than for surgery after aneurysm rupture (85% to 95%).
2 Aneurysms that are identified incidentally on CTC and are not large enough for elective surgery are followed with serial imaging to assess stability. The recommendation of the United States Preventive Services Task Force is to perform one-time screening for AAA by ultrasonography in men between the ages of 65 and 75 years who have ever smoked.
3 Screening programs for AAA using ultrasonography have demonstrated that almost 5% of men at age 65 have an asymptomatic AAA,
4 and that screening has effectively reduced the incidence of ruptured aneurysms by 49%.
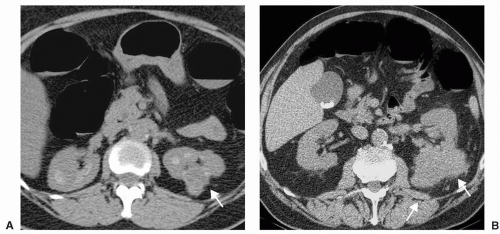
5Extracolonic malignancies such as renal cell carcinoma (RCC) or ovarian carcinoma that are discovered incidentally on CTC may be found at an earlier stage when they are more likely to be curable (see
Figure 8.2). Tsui et al. studied the prognostic significance of incidentally discovered RCC retrospectively in 633 consecutive patients. The authors found that patients with incidentally detected RCC had significantly lower grade and stage than tumors producing symptoms, leading to better patient survival and decreased recurrence. The 5-year survival rate was 85% for incidentally discovered RCC compared to 63% for symptomatic tumors.
6Although some extracolonic carcinomas that are discovered may not be operable or curable, they may be found when the patient is asymptomatic and still able to plan knowledgeably for their future before the onset of significant symptoms. Early discovery of disease with timely intervention could prevent the high cost of health care due to prolonged hospitalization
or extensive diagnostic and surgical procedures from later presentation of disease. Similarly if metastases are identified at the time of diagnosis of colon carcinoma on CTC, this can help direct patient management without additional diagnostic evaluation or intervention.
DISADVANTAGES
The investigation and treatment of incidental lesions that are ultimately found to be benign may be associated with increased health care costs, increased patient morbidity or mortality, and unnecessary radiation exposure to patients. Additionally, patients often experience anxiety and inconvenience associated with the discovery and workup of incidental findings. These disadvantages must be offset by the gains that may arise from the early detection of clinically important or malignant incidental lesions on CTC. Cost-effectiveness as estimated by the number of life years saved due to incidental lesions is yet unknown. The negative effect on patient well-being has been difficult to assess for CTC.
7 However, in a parallel study by Lerman et al. there was significantly increased anxiety in women who underwent additional evaluation of suspicious mammographic findings for breast lesions that were later found to be benign.
8 With continuing increases in image utilization in health care, the discovery of clinically unimportant findings will rise, and outcome studies will need to further explore cost effectiveness and direct benefits to patients.
COMPUTED TOMOGRAPHY COLONOGRAPHY TECHNIQUE
The CTC technique uses thin sections (≤5 mm, preferably ≤3 mm) and small reconstruction intervals (≤2 mm) allowing for the detection of colorectal polyps as well as well as extracolonic lesions.
9 Axial images are primarily used to examine for extracolonic findings. Multiplanar reformats are often helpful for further evaluation of questionable lesions identified on the axial views. CTC allows visualization of the lung bases as well as structures in the abdomen and pelvis. A soft tissue window (width 400, level 40) should be used for evaluation of the solid organs and most structures in the abdomen and pelvis. Lung windows (width 1,500, level -700) should be
used to examine the lung bases. Bone windows (width 2,000, level 300) should be used to examine the skeletal system.
Standard CTC technique requires supine and prone scanning which increases radiation dose. Many multidetector computed tomography (MDCT) colonography protocols employ low tube currents (≤100 mAs) to decrease radiation dose. However, even with these lower dose protocols, detection of extracolonic pathology is feasible. Iannaccone et al. evaluated ultra low-dose CTC and was able to successfully detect colorectal polyps and cancers using 10 mAs resulting in a 40% to 70% decrease in radiation dose compared with prior studies.
10 Although low mAs may not compromise the ability to detect colorectal polyps and cancers because of the inherently high contrast between the gas-filled lumen and the soft tissue density of the colonic wall, increased image noise will decrease the ability to evaluate for extracolonic lesions, particularly of the solid organs. More studies are needed to define the ability to detect extracolonic findings on CTC with decreasing radiation dose.
CLASSIFICATION OF EXTRACOLONIC FINDINGS
Extracolonic findings may be classified according to their clinical importance (see
Table 8.2). Site-specific differences in the classification of lesions are possible. The size and/or location of a lesion may impact on its classification.
Findings of major importance are defined as those requiring prompt or immediate additional evaluation, including further diagnostic imaging, surgery, or medical attention. Examples of these include AAA defined as an infrarenal aorta measuring >3 cm,
11 solid masses in abdominal organs, indeterminate pulmonary nodules, adenopathy, suspected bony metastases (see
Figures 8.3,
8.4 and
8.5). Pneumothorax, pneumonia, and pneumoperitoneum are of major importance and should be immediately communicated to the referring physician. Evidence of acute infection or inflammation such as pancreatitis, diverticulitis, and appendicitis are major findings that require immediate medical attention.
Findings of moderate importance are defined as those that are likely benign but may require additional evaluation or treatment in the future, such as cholelithiasis and nephrolithiasis (unless obstructing then major), enlarged ovary or uterus, splenomegaly (unless massive then major), cardiomegaly, and pleural effusion (see
Figures 8.6,
8.7,
8.8,
8.9 and
8.10). Uncomplicated ventral, inguinal, or other hernias are of moderate importance unless large and may be classified as of major importance if surgical or medical treatment may be necessary.