Examination Prerequisites
Judy Yee
Computed tomographic (CT) scanners, computer workstations, and graphic software for computed tomographic colonography (CTC) have undergone significant technologic advances over the last 10 years. However, the diagnostic ability of this test still relies on two key examination prerequisites. The colon must be well cleansed and well distended in order to obtain images that are optimally diagnostic. The presence of fluid or solid stool in the colon can compromise the accuracy of CTC and result in both missed lesions and false positives. Suboptimal distension or collapse of the colon can also cause lesions to be overlooked and may also simulate the stenosis of an annular carcinoma. Dual position (supine and prone) scanning is performed so that regions of the colon that have retained material or poor distension on one view may show improved cleansing or distension in the opposing position.
COLONIC CLEANSING
Cleansing of the colon is currently still necessary for CTC. Poor cleansing has been shown to decrease the sensitivity of CTC for the detection of polyps of all sizes.1 Polyps and cancers may be hidden in residual fluid pools or obscured by large amounts of retained solid material (see Figs. 2.1, 2.2, 2.3 and 2.4). Solid stool may also be mistaken for a sessile polyp, particularly if it is homogeneous in appearance on the two-dimensional CT images and adherent to the colon wall (see Fig. 2.5).
The protocol used for colonic preparation for CTC consists of two parts. The first part requires that the patient undergo dietary limitation and maintain a clear liquid diet starting 24 hours before the CT scan. The second part requires that the patient ingest a laxative that stimulates evacuation of colonic contents. The agents used for bowel cleansing for CTC are similar to those employed for other colon tests such as barium enema and standard colonoscopy. Saline cathartics such as sodium phosphate and magnesium citrate are highly osmotic agents that contain inorganic ions that cause shifting of fluid into the bowel lumen to stimulate peristalsis and emptying of the colon. Polyethylene glycol is an electrolyte lavage solution that is ingested in large volumes causing evacuation of the colon.
Sodium Phosphate
Sodium phosphate (also called phosphosoda) is often employed as a cathartic agent before barium enemas and colonoscopy. It is also one of the laxatives used for bowel cleansing before CTC. The osmotic effects of sodium phosphate cause large outflow from the colon. Sodium phosphate is available in a 45-mL (1.5 oz) bottle either alone or in a kit also containing four (5 mg) bisacodyl tablets and one (10 mg) bisacodyl suppository. Bisacodyl acts as a contact laxative and stimulates parasympathetic reflexes to increase bowel peristalsis.2
On the day preceding the CTC, patients are instructed to mix 45 mL (1.5 oz) of sodium phosphate with 120 mL (4 oz) of cool water, which is ingested with an additional 240 mL (8 oz) of water at approximately 5 P.M. It takes approximately 1 hour for the laxative effect to occur and patients are requested to stay near a rest room. Approximately 3 hours later at 8 P.M. the patient ingests the four bisacodyl tablets that take effect after approximately 6 to 12 hours. The bisacodyl suppository is placed in the rectum on the morning of the CT procedure and takes approximately 15 minutes for onset of effect. Patients should be instructed to keep the bisacodyl suppository in a cool environment until ready for use since it may easily melt if kept in a pocket for transporting to the imaging site for patient use.
Sodium phosphate is referred to as a dry preparation agent because it leaves little residual fluid in the colon. This can occasionally cause solid material to adhere to the bowel wall in the environment of a dry colon that may simulate a polyp on CTC. Many studies have been performed comparing the efficacy of sodium phosphate versus polyethylene glycol for colonic cleansing before colonoscopy. Some of the published trials have found both purgatives to result in similar bowel cleansing.3, 4 and 5 However, other studies have found sodium phosphate to cleanse the colon more effectively than polyethylene glycol.6, 7 and 8 In a meta-analysis that included
eight studies evaluating the effectiveness of sodium phosphate versus polyethylene glycol for cleansing the colon for colonoscopy in a total of 1,286 patients, it was found that there was no statistically significant difference in the quality of bowel cleansing between the two laxatives. However, sodium phosphate was better tolerated by patients and less costly, at a saving of approximately $40 per colonoscopy procedure.9 In a prospective, blinded randomized trial comparing oral sodium phosphate and polyethylene glycol solutions for bowel preparation before barium enema, no difference was identified in the amount of residual fluid and adequacy of colonic wall coating.10
eight studies evaluating the effectiveness of sodium phosphate versus polyethylene glycol for cleansing the colon for colonoscopy in a total of 1,286 patients, it was found that there was no statistically significant difference in the quality of bowel cleansing between the two laxatives. However, sodium phosphate was better tolerated by patients and less costly, at a saving of approximately $40 per colonoscopy procedure.9 In a prospective, blinded randomized trial comparing oral sodium phosphate and polyethylene glycol solutions for bowel preparation before barium enema, no difference was identified in the amount of residual fluid and adequacy of colonic wall coating.10
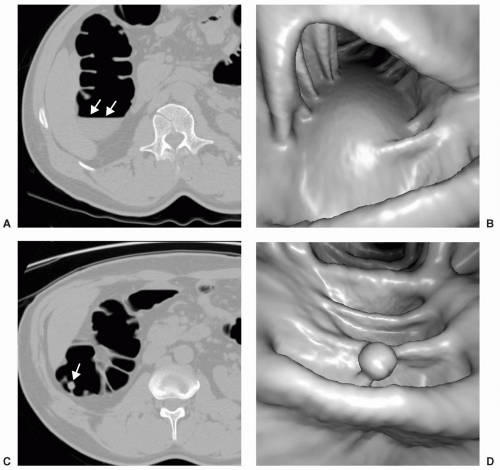 FIGURE 2.1 Layering fluid along the posterior wall of the hepatic flexure on this supine axial view (A) and on the three-dimensional endoluminal image (B). The fluid has shifted to reveal a pedunculated polyp on the prone axial view (C) and on the corresponding 3D view (D). |
Complications due to the administration of sodium phosphate are uncommon. However, patients may become hypovolemic, and occasionally severe electrolyte abnormalities may occur including hypernatremia, hyperphosphatemia, hypocalcemia, and hypokalemia.11,12 The administration of sodium phosphate is contraindicated in patients with renal failure, history of electrolyte disturbances, congestive heart failure, ascites, ileus, and bowel obstruction.13 Patients on diuretic medications should also not receive sodium phosphate. Two doses of sodium phosphate have been prescribed by some physicians and called a double dose, consisting of a total volume of 90 mL (3 oz) for bowel cleansing before CTC. One dose is given the evening before the procedure and the second dose is given the morning of the procedure with each dose separated by 10 to 12 hours.14 Particular caution must be exercised with the use of double dose phosphosoda, given the potential for serious electrolyte abnormalities particularly in the elderly. A warning has been issued by the U.S. Food and Drug Administration (FDA) regarding the potential toxicity of taking sodium phosphate as a bowel cleansing agent before colonoscopy.15 Recently, the packaging of over-the-counter sodium phosphate was modified in the United States so that a single volume bottle of 90 mL (3 oz) is no longer available. Patients with significant comorbid clinical conditions are advised to avoid the use of sodium phosphate.16
Magnesium Citrate
Magnesium citrate is also classified as a saline laxative. It may be employed for bowel cleansing for CTC.
Magnesium citrate acts by both preventing resorption of fluid and by stimulating cholecystokinin, which in turn causes small bowel fluid secretion, increased peristalsis and emptying.17 Magnesium citrate comes packaged in a powder form that the patient reconstitutes with 240 mL (8 oz) of water or as a 300-mL (10-oz) bottle containing a premixed solution ready for ingestion. A typical bowel-cleansing protocol consists of ingestion of magnesium citrate in the late afternoon of the day before the CT at approximately 5 P.M. It is then followed by ingestion of an additional 240 mL (8 oz) of water and the patient is instructed to maintain hydration during the evacuation process. Four bisacodyl tablets and a suppository are administered in addition to the magnesium citrate preparation as described in the preceding text for the sodium phosphate preparation protocol.
Magnesium citrate acts by both preventing resorption of fluid and by stimulating cholecystokinin, which in turn causes small bowel fluid secretion, increased peristalsis and emptying.17 Magnesium citrate comes packaged in a powder form that the patient reconstitutes with 240 mL (8 oz) of water or as a 300-mL (10-oz) bottle containing a premixed solution ready for ingestion. A typical bowel-cleansing protocol consists of ingestion of magnesium citrate in the late afternoon of the day before the CT at approximately 5 P.M. It is then followed by ingestion of an additional 240 mL (8 oz) of water and the patient is instructed to maintain hydration during the evacuation process. Four bisacodyl tablets and a suppository are administered in addition to the magnesium citrate preparation as described in the preceding text for the sodium phosphate preparation protocol.
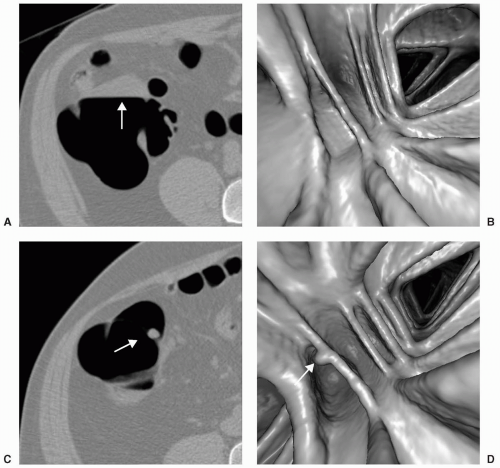 FIGURE 2.2 Prone axial image (A) and endoluminal view (B) shows residual fluid along the dependent wall. In the supine position, a sessile polyp is apparent on the axial image (C) and endoluminal image (D) in the same area that was obscured by fluid in the prone position. |
Magnesium citrate may be preferred over sodium phosphate in patients who are at risk for electrolyte disturbances. Magnesium citrate is a saline cathartic, but contains much less sodium than sodium phosphate. In its mixed form, magnesium citrate has 12 mg of sodium whereas sodium phosphate contains 5,004 mg of sodium. Magnesium citrate has not been found to cause the same severe electrolyte abnormalities that have been found associated with sodium phosphate. In a study comparing patients who received either magnesium citrate or sodium phosphate, all patients receiving the sodium phosphate preparation were found to have hyperphosphatemia followed by hypocalcemia.18 A combination of magnesium citrate with a smaller volume of polyethylene glycol has been used successfully as a cleansing regimen for colonoscopy. This was found to improve cleansing and to shorten preparation times.19
COLONIC DISTENSION
The colon must be adequately distended in order to allow for the detection of the lesion and to minimize the potential for false-positive lesions (see Figs. 2.6, 2.7 and 2.8). Poor distension of a segment of colon may have an appearance similar to an annular carcinoma causing luminal narrowing, particularly on the three-dimensional
view (see Fig. 2.9). Focal thickening of folds in an area of suboptimal distension may appear polypoid, particularly on two-dimensional images.
view (see Fig. 2.9). Focal thickening of folds in an area of suboptimal distension may appear polypoid, particularly on two-dimensional images.
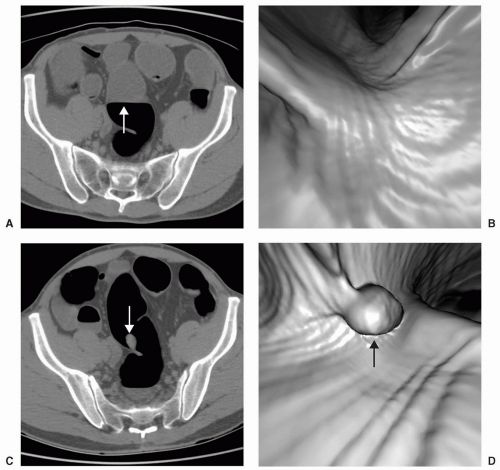 FIGURE 2.3 Large amount of residual fluid is present in the sigmoid colon on the prone axial (A) and 3D images (B). A large pedunculated polyp is detected in the supine view on axial (C) and 3D views (D) after the large fluid pool has moved away. This patient received polyethylene glycol for bowel preparation. |
HOW TO INSUFFLATE THE COLON
After the patient is placed on the CT table, a rectal tube is inserted for the administration of either room air or carbon dioxide to distend the colon. Placement of the rectal tube may be performed by a trained physician, technologist, or nurse, based on local guidelines. The tip is easily inserted into the rectal vault with the patient in a right side-down decubitus position. Rectal tip placement is facilitated by use of a small amount of lubricant gel. The holes of the rectal tip may become obstructed if too much gel is applied. Lidocaine gel may be used if the patient has anorectal pain or if there is evidence of external hemorrhoids. There are a variety of administration sets that may be used for manual insufflation of gas for CTC. A simple soft rectal tip attached to tubing with an insufflation bulb at the end is adequate and inexpensive. A Foley catheter may also be used, attached to an insufflation bulb.
The colon is insufflated with the patient initially in the right side-down decubitus position, which allows filling of the descending colon and the rectosigmoid. The patient is then rotated into the supine position and additional gas is administered to completely fill the transverse colon and then the right colon. Typically at least 3 L of gas is needed to obtain sufficient colonic distension, and additional gas is required if the patient has difficulty with gaseous retention. Some radiologists will inflate the rectal balloon in order to aid in gaseous and tube retention. However, caution is advised to clear the rectal vault of any lesion first, by performing a rectal examination to help avoid the possibility of causing perforation or significant
bleeding. Adequate distension may be obtained in most patients without the use of an inflated rectal balloon.
bleeding. Adequate distension may be obtained in most patients without the use of an inflated rectal balloon.
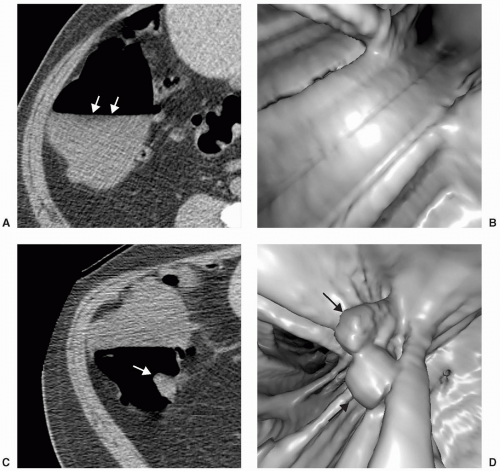 FIGURE 2.4 A patient who received polyethylene glycol bowel-cleansing regimen demonstrates a large amount of retained fluid seen in the ascending colon on the supine axial (A) and 3D views (B). A polypoid mass that was found to be malignant is revealed on the supine axial (C) and 3D views (D) when the fluid falls along the dependent wall. |
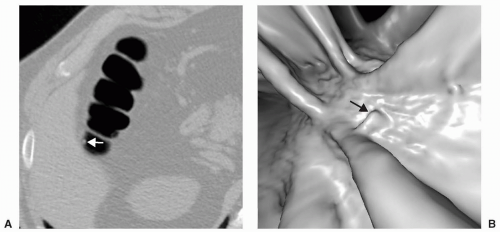 FIGURE 2.5 Supine axial image shows a small polypoid lesion (A). The endoluminal image demonstrates the linear, angular appearance of this lesion that is characteristic of stool (B). |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


