Evaluation of Resection Specimens
General Comments
The unopened bowel should be carefully examined upon receipt from the operating room, then opened and pinned to a corkboard for fixation in 10% buffered formalin. Those specimens that are received partially opened or, worse yet, received in formalin unopened and allowed to fix over a weekend tend to become fixed in distorted positions, making it extremely difficult to establish normal anatomic relationships as well as the various pathologic features that are present. In the worst case, one may have extreme difficulty determining the exact anatomic location of a tumor and in obtaining accurate measurements to the nearest resection margins.
Inspection of the unopened bowel provides important information. Dilation is indicative of obstruction, and it informs the examiner that the dilated portion is the proximal part of the specimen. Retraction of the serosal surface in the region of a palpable mass indicates serosal invasion (Fig. 14.82). Palpation of the serosal surface discloses the circumferential extent of the tumor so that one can avoid transecting the tumor when opening the bowel, unless it is completely annular. The mesentery and pericolonic fat should be carefully examined for lymph nodes and evidence of gross vascular invasion. Those extensively involved by metastases are enlarged, hard, and white on cut surface. Grossly, venous invasion may be evident.
The surgical specimen should be opened along the antimesenteric border, unless palpation of the specimen indicates that a tumor lies in this area, in which case the bowel should be opened taking care to avoid sectioning through the middle of the tumor. The resection specimen should be described, particularly with respect to the distance to the nearest margins, if these are close to the tumor. After having been opened, cleaned, and described, the specimen is pinned to a corkboard and immersed floating upside down in formalin for a number of hours to obtain adequate fixation. The specimen should be photographed. This can be done when it is received fresh or following fixation. Some details become more obvious after the fixation.
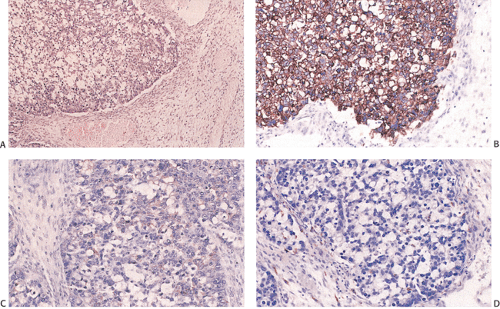 FIG. 14.153. Colon carcinoma metastatic to ovary. A: The ovary contains a poorly differentiated mucinous adenocarcinoma. B: Cytokeratin-20 immunostains are strongly positive. C: Immunohistochemical staining for cytokeratin-7 is negative. D: Negative HAM56 staining. |
Evaluation of Tumor Margins
One could question whether there is any justification for the routine histologic examination of bowel resection margins in colorectal carcinoma resection specimens, particularly large colectomy specimens in which the extent of the surgical resection is determined by the vascular supply. Most tumors rarely extend >1.5 cm laterally in the bowel wall unless the tumor has a mucinous histology. Certainly any tumor that is >5 cm from the nearest margin, is not poorly differentiated, and does not have a mucinous or signet ring histology is not likely to involve the tumor margins. What is more important is the examination of the degree of intramural spread of the tumor. This is particularly true for rectal cancers that lie below the peritoneal reflection. The deep radial margins represent an important prognostic indicator and should be evaluated carefully. In order to adequately assess the radial margins, the specimen should be inked at the time it is received.
Lymph Node Examination
Tumor stage is the single most important prognosticator for patients with colorectal carcinoma; therefore, an attempt to identify nodal metastases is very important in handling the resection specimen. The nodes most likely to become involved are those closest to the tumor. Pericolic lymph nodes may be obtained in one of several ways. The fat adjacent to the colon (the mesocolic fat) can be meticulously dissected off the muscularis propria and then searched by a variety of techniques (see below), or a rim of immediately adjacent fatty tissue may be left on the specimen with the sections taken in such a way as to include this fatty tissue. Since the nodal metastases occur progressively from those closest to the tumor to those most distant from it, these are the most likely to be positive. As noted in the TNM staging system (Table 14.16), the number of positive lymph nodes distinguishes the N status.
There are several ways to search for minute lymph nodes in resection specimens for adenocarcinoma. Lymph nodes can be removed from the fresh or fixed specimen, or the fatty tissues can be placed in a clearing solution. Using a clearing technique, metastases are found in 45% to 78% of small lymph nodes measuring <5 mm in diameter (535,826,827). Detection of these small lymph nodes containing metastases is important in accurately staging rectal carcinomas (827). Several groups identified a significantly greater number of nodes and a greater number of lymph nodes with metastases in the cleared specimens compared with noncleared specimens (828,829,830). Traditional dissection showed metastases in 43.7% of patients, but after fat clearance a further 4.8%
were found to be lymph node positive (828). Unfortunately, clearing techniques increase the turnaround time for the resection signout. However, in contrast, Jass et al (831) found no significant difference in the number of lymph nodes harvested when traditional dissection and fat clearance methods were compared. The difference in the number of lymph nodes found by traditional dissection versus those found during clearing depends, of course, on the meticulousness with which the initial dissection is done.
were found to be lymph node positive (828). Unfortunately, clearing techniques increase the turnaround time for the resection signout. However, in contrast, Jass et al (831) found no significant difference in the number of lymph nodes harvested when traditional dissection and fat clearance methods were compared. The difference in the number of lymph nodes found by traditional dissection versus those found during clearing depends, of course, on the meticulousness with which the initial dissection is done.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


