Erectile Dysfunction and Other Urological Issues in the Transplant Patient
Erectile Dysfunction and Other Urological Issues in the Transplant Patient
Sean P. Van Zijl
Benjamin H. Lowentritt
Geoffrey N. Sklar
Division of Urology, University of Maryland School of Medicine, Baltimore, Maryland 21201
INTRODUCTION
Genitourinary complications commonly affect the renal transplant population. Although a minority of transplant surgery is currently performed by urologists, the preoperative evaluation and postoperative complications frequently require urological input. Posttransplant erectile dysfunction (ED), in particular, constitutes a major morbidity in this population. A thorough understanding of the urological issues involved and the diagnostic and therapeutic options available enables an effective multidisciplinary approach to the transplant patient. This chapter focuses on ED and other specific urological issues these patients may experience.
EPIDEMIOLOGY OF ERECTILE DYSFUNCTION
In the 1988 consensus conference, the National Institutes of Health replaced the term impotence with the broader term erectile dysfunction. ED was defined as the consistent inability to maintain a penile erection sufficient for adequate sexual relations. ED ranks as one of the most common medical conditions (1). This is especially true for the transplant population. Sexual dysfunction ranks among the 10 symptoms most frequently reported prior to transplant and it is also the least responsive to the success of the transplant (2).
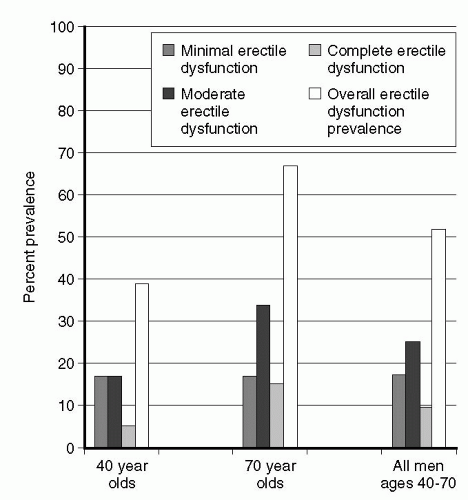
The major epidemiologic study of the prevalence of ED in the United States was the Massachusetts Male Aging Study (MMAS). This study defined the risk factors for the development of ED. Feldman et al reported on the prevalence of impotence in a general population of men 40 to 70 years old (Fig. 30.1) (3). Based on this data and a projection of the United States population projection, ED will affect more than 25 million men, age 40 to 70 by the year 2005, and millions older than 70 years (4). Age was the variable most strongly associated with ED in the MMAS (3). Estimated prevalence rates were 39% in men 40 and 67% in those 70 years old. Additionally, this study also suggested a higher probability of ED in association with certain treatable medical conditions (3). After adjusting for patient age the probability of complete ED was 39% in men with treated heart disease, 28% with treated diabetes, and 15% with treated hypertension versus 9.6% in the entire population surveyed. Furthermore, the probability of ED in these diseases was further increased in patients who smoked cigarettes. For instance, the probability of complete ED was 21% in nonsmoking individuals with treated heart disease compared with 56% in smokers with treated heart disease (5). It can safely be stated that even if cigarette smoking itself is not a risk factor for ED, it has an additive effect when associated with other modifiable risk factors (Table 30.1). Additionally the presence and degree of depression correlated with ED (3).
Fig. 30.1. Prevalence of erectile dysfunction. (Adapted from Feldman HA, Golstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994;151:54-61, with permission.)
TABLE 30.1.Modifiable and nonmodifiable risk factors for the development of erectile dysfunction
Various medications and substances of abuse are commonly associated with ED (6). The incidence of drug related ED may be as high as 25% (7). Drugs that may cause ED include certain antihypertensive medications, hormones, antidepressants, tranquilizers, alcohol, tobacco, heroin and cocaine. The incidence of ED in patients receiving various types of antihypertensive drugs was examined in the Treatment of Mild Hypertension Study (8,9). The incidence of ED ranged from 2.8% in the alpha-blocker group to 15.7% in the diuretic group compared with 4.9% in the placebo group (9).
The most common organic etiology of ED is vascular, which is associated with atherosclerosis, endothelial dysfunction and diabetes mellitus. Atherosclerotic disease is the cause of approximately 40% of ED in men older than 50 years (10). In patients with diabetes the prevalence of ED is approximately 50%, dependent on patient age, duration and severity of diabetes (11). In addition to affecting small vessels, diabetes may affect the cavernous nerve terminals and endothelial cells, resulting in a deficiency of neurotransmitters (11). Chronic renal failure has been associated with diminished erectile function. In one study, by the time patients with uremia began maintenance dialysis, 50% were impotent (12). In another study, 78% of the patients were found to have cavernosal artery occlusive disease and 90% to have venoocclusive dysfunction (13). The mechanism is probably multifactorial: hypogonadism with elevation of prolactin levels, diabetes mellitus, vascular insufficiency, multiple medications, autonomic and somatic neuropathy, and psychological stress (14).
Malavaud et al published a cross-sectional study of male transplant recipients and estimated the transplant ED prevalence at 55.7% with a mean age of 48.5 years (2). This is significantly higher than in a diverse population, as reported in the National Health and Social Life Survey (NHSLS) showing a prevalence of 11% in the 40 to 49 years age group and 18% in the 50 to 59 years age group. After successful renal transplantation, 50% to 80% of patients returned to their pre-illness potency (15). In our own patient population at the University of Maryland, the incidence of ED in the posttransplant patient is approximately 53%. Of these, approximately 75% resume normal sexual function after treatment.
ERECTILE ANATOMY AND PHYSIOLOGY
ED has been recognized as a medical phenomenon for at least two epochs, but only in the last 20 years has the complexity of erectile pathophysiology been appreciated (16). Every physician who treats patients with ED should have a basic understanding of the processes that cause erection and detumescence.
Anatomy
The penis is composed of two paired corpora cavernosa and the corpora spongiosum surrounding the urethra. The corpora are spongy bodies that house a complex of fibroelastic tissue and sinusoids (Fig. 30.2). An erection is caused by increased blood flow to the corpora and decreased venous outflow. As blood flows in, the sinusoidal spaces expand and this stretches and alters the laminal components of the tunica albuginea. Corporal expansion causes deviation of the emissary veins and decreases venous outflow, further elevating corporal pressure. Contraction of the arteriolar smooth muscle causes reduced corporal blood flow and eventual detumescence. Penile blood flow originates from the pudendal branch of the internal iliac artery (17).
FIG. 30.2. Penile anatomy. (From Lue TF. Physiology of penile erection and pathophysiology of erectile dysfunction and priapism. In: Walsh PC, Retik AB, Vaughn ED, Wein AJ, eds. Campbell’s uology. Philadelphia: Saunders, 2002.
Neurology of Erection
Penile innervation is complex and a detailed discussion is beyond the scope of this text. The innervation of the penis is both autonomic and somatic. Sympathetic fibers originate at the T10-T12 spinal level. They pass through the sympathetic chain and join the pelvic plexus. Parasympathetic fibers originate from the S2-S4 levels and coalesce within the pelvic plexus. The cavernous nerve carries the autonomic fibers from the pelvic plexus to the penis. The sympathetic nerves release norepinephrine at the final synapse, which causes cavernosal smooth muscle contraction. The parasympathetic fibers release nitric oxide (NO) and several other transmitters to cause smooth muscle relaxation (17).
Somatic innervation is comprised of afferent sensory nerves and efferent motor nerves that control the bulbocavernosal and ischiocavernosal muscles. Somatomotor innervation originates in Onuf’s nucleus and is transmitted to the penis via the pudendal nerve. This innervation is the basis of the bulbocavernosal reflex arc (17).
Neurotransmission of Erections
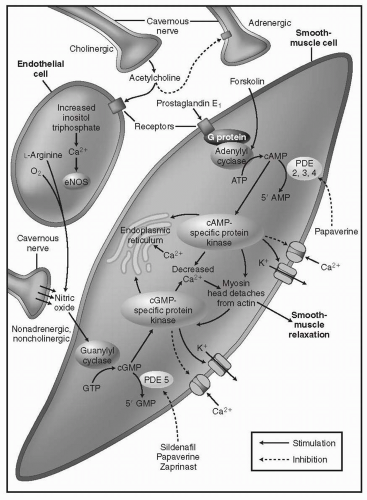
The biochemistry of erectile function involves a complex interaction of numerous neurotransmitters. Presented is a very simplified version that will allow a basic understanding. Erections are caused by the release of NO from parasympathetic nerves (nonadrenergic, noncholinergic [NANC]) and endothelial cells (17). NO induces the formation of cyclic guanosine monophosphate (cGMP) by activating guanylate cyclase. cGMP causes a decrease in intracellular Ca2+ through various pathways, resulting in smooth muscle relaxation (17,18). Acetylcholine also acts on this pathway by inhibiting adrenergic neurons, and inducing endothelial cells to produce NO. Detumescence is caused by a decrease in NO release, sympathetic discharge after ejaculation, and a breakdown of cGMP by phosphodiesterase 5 (PDE-5). Flaccidity is maintained primarily by sympathetic discharge of norepinephrine acting on the α-adrenergic receptors of cavernosal smooth muscle (Fig. 30.3) (17).
ETIOLOGY OF ERECTILE DYSFUNCTION IN THE TRANSPLANT PATIENT
Renal transplant patients have all suffered from uremia. They have frequently spent a significant amount of time on dialysis and often have other comorbidities including hypertension and diabetes. Although a successful transplant may improve erectile function and return libido, in many cases some degree of sexual dysfunction may persist (2).
The major organic etiologies of ED are presented in Table 30.2. Many cases of ED are of combined etiologies, especially in transplant patients. Purely psychogenic impotence is believed to account for 20% to 30% of causes of ED but psychogenic issues are present in a majority of ED patients even with organic etiologies (19).
FIG. 30.3. Neurotransmitters of erection. (From Lue TF. Physiology of penile erection and pathophysiology of erectile dysfunction and priapism. In: Walsh PC, Retik AB, Vaughn ED, Wein AJ, eds. Campbell’s urology. Philadelphia: Saunders, 2002, with permission.)
Vasculogenic Etiologies
Vascular causes of ED occur in most patients with ED. Transplant patients, especially those with diabetes and hypertension may have an increased frequency of cholesterol plaques and accelerated plaque formation. Hyperlipidemia contributes to plaque formation and is seen frequently in diabetic and transplant patients (20). Hyperlipidemia and diabetes can also affect erections on the microvascular level by adversely effecting endothelial relaxation. Smoking not only is a factor for atherosclerosis, but also reduces blood flow to the penis and reduces production of NO (20). Transplant patients may also have reduced blood flow to the pudendal artery if the internal iliac is used in an end-to-end anastomosis to the allograft (21,22). Transplant recipients with ED have a 68% incidence of venoocclusive dysfunction compared to a 26% incidence in potential transplant recipients (22).
TABLE 30.2.Etiology of erectile dysfunction
Vasculogenic
70%
Pharmacologic
10%
Endocrinologic
4%
Neurologic
5%
Iatrogenic/trauma
11%
(Adapted from Brock GB. Issues in the assessment and treatment of erectile dysfunction: individualizing and optimizing therapy for the “silent majority.” Rete Biomedical Communications Corp. http://www.medscape.com, with permission. accessed September, 2002)
Neurogenic Etiologies
Classically, neurogenic causes like spinal cord injuries create an imbalance between the competing sympathetic and parasympathetic forces. Hypertension and coronary artery disease cause increased sympathetic outflow and this acts on the penis by maintaining smooth muscle contraction and attenuating any vasodilatation brought about by NO or acetylcholine. Injury to the cavernosal nerves either from surgery (radical retropubic prostatectomy, cystectomy, and surgery on the rectum) or radiation therapy can result in profound ED.
Endocrinologic Etiologies
Endocrinopathies are an infrequent but recognized cause of ED. Diabetics have been shown to have decreased NO production and disturbance of the erectile sensory and autonomic reflex arcs. Nitrogenic nerves have been shown to be selectively degenerated in diabetic rats (23,24). Men with a longer duration of diabetes also have a higher incidence of ED. Romeo et al have shown an inverse relation between glycemic control and ED development (23). It is felt that advanced glycosylation products contribute to ED by impairing cavernosal relaxation by inactivating NO and by generating superoxide anions (24). Additionally, hypothyroidism as well as adrenal insufficiency may contribute to ED (16). The pathophysiology, evaluation, and treatment of transplant patients with ED and hypogonadism are discussed later in this chapter.
Chronic Disease
Several chronic disease states can contribute to the development of ED and deserve further discussion. Chronic renal failure (CRF) affects erectile function through several mechanisms. A study by Kaufman et al revealed arterial insufficiency in 78% of patients with impotence and CRF (13). Ninety percent of the patients also had venoocclusive dysfunction. Patients who were transplanted early in their disease course seemed to display much less vascular insufficiency (13). Hypoxia associated with CRF is another possible explanation for the high rate of impotence. Pulmonary microemboli or anemia may result in hypoxia, which has been shown to down regulate NO production and to increase smooth muscle tone. Hypoxia may also contribute to the penile fibrosis seen in patients on dialysis. Correction of anemia with erythropoietin has been shown to increase sexual function in these patients. NO synthase inhibitors have also been shown to be elevated in patients with CRF (13).
The duration and severity of hypertension has been associated with the incidence of ED. Hypertension induces structural changes such as intimal thickening of vascular beds (25). Additionally, pharmacologic control of hypertension induced a 12% regression in penile vascular structure thereby reducing arterial resistance. This effect was most pronounced for angiotensin-converting enzyme (ACE) inhibitors (26,27).
EVALUATION OF ERECTILE DYSFUNCTION IN THE TRANSPLANT PATIENT
Due to the high incidence of ED in the transplant patient population and the negative impact of this on patients’ quality of life, it is incumbent on the physician to initiate the discussion about sexual function. Patients still fear embarrassment or apathy from their physicians and are reluctant to reveal their concerns. It is estimated that at least 70% of ED is undiagnosed and only 12% of patients with ED are treated (19).
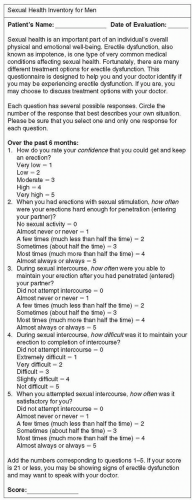
Introduction of the subject can be accomplished with simple open-ended questions or by using questionnaires. The Sexual Health Inventory for Men (SHIM) presented in Figure 30.4 is based on the clinically validated International Index of Erectile Function (IIEF). Questionnaires allow a rapid communication of the problem in a nonthreatening way, bringing the problem immediately to the attention of the physician.
History and Physical
As with most other medical conditions, a good history and physical will go a long way in establishing the diagnosis and likely etiology of the patient’s ED. Basic laboratory testing and physical exam increases the diagnostic rate of ED to 80% (28).
The history should encompass several elements relevant to ED:
Presence of coronary artery disease and any history of myocardial infarction
Presence of any chronic illnesses such as diabetes, hypertension, dyslipidemias, and hormonal abnormalities
Surgical history focused on prior pelvic surgery (i.e., transplant grafts and their anastomoses, radical prostatectomy)
Psychiatric history, including any medications, hospitalizations, and the presence of suicidal ideation or depressed mood
Pelvic trauma or pelvic radiation (i.e., brachytherapy or colonic irradiation)
The history should also include a specific sexual history that includes:
Type of relationship (i.e., monogamous)
Chronicity of the ED
Presence or absence of morning erections
Premature ejaculation or difficulty ejaculating
Painful erections
Presence of penile curvature during erection
Is the patient able to masturbate?
FIG. 30.4. Sexual health inventory for men.
TABLE 30.3.Medications implicated in erectile dysfunction
Antihypertensives
Names
β-Blockers
Propranolol
Labetalol
α-Blockers
Doxazosin
Prazosin
Terazosin
Phenoxybenzamine
Sympatholytics
Clonidine
Methyldopa
Reserpine
Guanethidine
Vasodilators
Hydralazine
Diuretics
Thiazides
Spironolactone
Acetazolamide
Amiloride
Chlorthalidone
HMG CoA reductase inhibitors
Lovastatin
Pravastatin
Simvastatin
Antidepressants
Serotonin reuptake inhibitors
Sertraline
Paroxetine
Tricyclics
Imipramine
Amitriptyline
Doxepin
Clomipramine
Desipramine
Monoamine oxidase inhibitors
Phenelzine
Isocarboxazid
Tranylcypromine
Clorgyline
Pargyline
Antipsychotics
Haloperidol
Phenothiazine
Risperidone
Antianxiety
Clonazepam
Diazepam
Antiandrogens
Flutamide
Bicalutamide
Anticonvulsants
Phenytoin
Carbamazepine
Miscellaneous
Indomethacin
Allopurinol
Prochlorperazine
H2 Antagonists
Ranitidine
Cimetidine
Famotidine
5α Reductase inhibitors
Finasteride
Luteinizing hormone-releasing hormone agonists
Leuprolide acetate
Zoladex
Once the history has been completed a focused physical examination should be performed. Physical exam rarely is able to diagnose the etiology of ED but rather provides valuable clues.
Laboratory Studies
Many of the laboratory tests performed for the evaluation of ED comprise part of the routine laboratory evaluation of the transplant patient. The following list comprises the tests that are ordered at our institution when seeing a transplant patient with ED:
Basic metabolic panel (glucose tolerance testing if glucose is elevated)
Testosterone (total-morning or total and free/bioavailable)
Most patients with ED can be successfully treated by their primary physicians. With this in mind, the Process of Care Model was developed by a multidisciplinary consensus panel with expertise in sexual health to facilitate the initial evaluation and treatment of men with ED (29).
After completing the initial history and physical exam, the practitioner should be able to characterize the severity of the ED as mild, moderate, or severe. The etiology should also be apparent as either psychogenic or organic (29). Most transplant patients have a mixed organic-psychogenic source of their ED.
At this stage the physician should also decide if referral to an appropriate specialist is warranted. Referral is indicated in:
Young patients with a history of pelvic trauma
Patients with endocrine abnormalities
Patients with anatomic defects such as Peyronie’s disease
Patients with psychiatric comorbidities
Patients who wish to have a more detailed diagnostic evaluation
Patients who have undergone treatment for prostate cancer
Prior to initiating any treatment, the physician needs to have a discussion with the patient and if possible his partner, to establish the treatment goals and preferences of the couple. Patients who have ED that does not respond to lifestyle modification and oral therapy should be classified as having complex ED and should be referred to a Urologist or other specialists for further workup and/or treatment (19).
Endocrine Evaluation
Testosterone has long been thought to be the hormone responsible for male sexual function, though a direct effect on erectile and sexual function is not completely clear (30). Furthermore, it is clear that hypogonadism cannot always be identified clinically by history or physical examination (31). Hyperprolactinemia from any cause results in both reproductive and sexual dysfunction. In most cases of ED, the treatment bears little relation to its etiology; however, with endocrine abnormalities, a disease-specific treatment may result in the restitution of potency (31).
It has been suggested that endocrine abnormalities account for anywhere from 2% to 23% of the cases of ED and 1 in 200 men has abnormally low testosterone levels (30,31). Testosterone levels decline naturally with age, and it is difficult to separate the age component of ED risk from that of low testosterone levels (3).
Patients with chronic renal insufficiency and those on hemodialysis suffer from abnormalities of the hypothalamic-pituitary-gonadal axis. Holdsworth et al studied uremic patients and found that maintenance hemodialysis was unable to correct their endocrine abnormalities and that sexual function was only minimally improved (32). They further found that successful transplantation led to corrections in the hypothalamic-pituitary-gonadal axis with subsequent improvement in sexual activity, normalization of testosterone, and sperm counts. A study by Saha et al demonstrated that hyperprolactinemia and hypogonadism in uremic patients were corrected with a successful renal transplant (33).
The initial endocrine evaluation of a transplant patient with ED should include testosterone and prolactin testing. A morning total testosterone level suffices in most patients; however, as men age this becomes less accurate. Fractionated testosterone, including measurement of total testosterone (240 to 950 ng/dL), free testosterone (9 to 30 ng/dl), and percentage of free testosterone (2% to 4.8%) are clinically available. Multiple drugs can adversely alter androgen levels and bioavailability (Table 30.4). Only men with clearly documented hypogonadism are candidates for testosterone replacement therapy. We prefer to refer patients with secondary hypogonadism to an endocrinologist for further work-up of possible pituitary or hypothalamic dysfunction.
TABLE 30.4.Drugs that affect androgen levels or effects
Inhibit testosterone production
Spironolactone
Common chemotherapeutic agents: methotrexate, alkylating agents
Ketoconazole
Metronidazole
Flutamide
Cimetidine
Cyproterone
Inhibit GnRH release/production
Progesterone
Estrogen
GnRH agonists (leuprolide, goserelin)
Elevated prolactin levels
Estrogen
Phenothiazines
Tricyclic antidepressants
Reserpine
Opioid analgesics
Cocaine
GnRH, gonadotropin-releasing hormone
Hyperprolactinemia is found in approximately 2.1% of the cases of ED. Johri et al demonstrated little relation between libido and prolactin levels (34). Their study showed that significant hyperprolactinemias were missed when relying on the complaint of low libido and serum testosterone measurement. For this reason we recommend an initial serum prolactin measurement. Prolactinomas are the most important cause of hyperprolactinemia, and though these are usually benign, they can cause significant morbidity. Prolactinomas are evaluated with computed tomography (CT) scans or magnetic resonance imaging (MRI) of the sella turcica. There are both medical and surgical treatments for prolactinomas. Medical treatment usually consists of a dopamine agonist, such as bromocriptine.
Successful renal transplants have been shown to correct many of the endocrine abnormalities in uremic patients (35,36). The etiology for ED in these patients is rarely solely caused by endocrine abnormalities. Therefore, treatment for hypogonadism should be initiated only after other noninvasive treatment modalities have been exhausted.
Treatment of Hypogonadism
Androgen replacement therapy has evolved over many years and now the patient and clinician have several options (Table 30.5).
Long-acting intramuscular injections are usually administered every 2 to 3 weeks. The injections do cause some discomfort, more so when given frequently. Oral testosterone has the advantage of ease of administration; however, it is limited by rapid hepatic metabolism. For this reason oral administration requires that the testosterone be alkylated and this carries a higher risk of liver toxicity. Testosterone undecanoate is a testosterone ester that is available outside the United States. It has been shown to have a much lower side-effect profile, and more predictable serum levels (36).
There are currently several transdermal preparations of testosterone clinically available. Transdermal patches were a major development in that they provide daily dosing and ease of administration. They are carefully engineered to approximate the diurnal variability of testosterone release. The first patches were applied to the scrotum and keeping the patch in place proved to be difficult leading to the development of nonscrotal patches. The most common side effects are contact dermatitis at administration sites. Recently, transdermal testosterone gels have become clinically available: Androgel (Unimed Pharmaceuticals, Marietta, Georgia) and Testim (Auxilium Pharmaceuticals, Norristown, Pennsylvania). These are usually applied to the arms or chest and achieve reliable serum levels within 24 hours (36).
Contraindications to hormonal therapy include known or suspected prostate cancer or breast cancer. Relative contraindications include sleep apnea, and polycythemia and edematous states. In men on testosterone replacement, PSA should be checked biannually for the first year, and then annually. Additionally, the patient should be followed with serial hematocrit testing as occasionally polycythemia does develop (36).
Psychiatric Factors of Sexual Dysfunction
Sexual dysfunction was once thought to be a primarily psychiatric disease. Often psychogenic sexual dysfunction is viewed as a diagnosis of exclusion once a medical evaluation has been completed. The treating physician should be aware that psychogenic components of ED are often present even in cases with a clear organic etiology. Failure to recognize this may result in unsuccessful treatment.
Psychiatric illness has been implicated in sexual dysfunction and ED. Results from the MMAS showed that 55% to 90% of men with ED had symptoms of depression and 50% to 90% of men with depression had ED (37). Lee et al found that the prevalence of psychiatric pathology in patients presenting with ED was 33% (38). Depression is the most common psychiatric disorder of patients with end-stage renal disease (ESRD) (39) and the prevalence of major depression or depressive symptoms in patients with ESRD ranges from 1% to 18% (40).
Transplant patients typically have a mixed organicpsychogenic ED. One study of sexual dysfunction in dialysis patients found that men who were able to achieve erections during clinic testing reported that they were totally impotent with their partners (41).
Many patients experience a return of libido and/or erectile function after they receive a successful allograft (32,42). Persistent causes of this ED are usually performance anxiety, lack of stimulation, or relationship conflicts. For performance anxiety, desensitization and anxiety reduction techniques are used. The presence of a partner can often bring to light issues that are best treated with either sexual or relationship counseling (43). Organic therapies such as sildenafil have very high success rates in psychogenic ED as well (43).
ED can also be caused by the treatment of psychiatric disorders. Ninety percent of the antidepressants currently used are selective or non-selective serotonin reuptake inhibitors (SSRIs) that can have numerous sexual side effects. A recent study showed that sildenafil significantly improved erectile function in men taking SSRIs (37). Failure by the physician to appreciate the large role that psychological factors play may lead to unsuccessful treatment of ED. Often transplant patients are best served with a combination of an organic therapy and psychiatric or sexual therapy (44,45).
Phosphodiesterase 5 Inhibitors
It would be very difficult to overstate the effect that the introduction of sildenafil citrate (Viagra) has had on the treatment of ED. In the 5 years since its release, sildenafil has become the first line treatment for ED regardless of etiology (45).
Sildenafil was first synthesized in England in 1989 as an antianginal, inhibiting phosphodiesterase type 5 (PDE-5), yielding relaxation of vascular smooth muscle. During safety trials, an interesting effect of improved erections was noted and research focused on its use in ED (46). Early trials in 1993 showed promise and prompted further investigation into sildenafil’s mechanism of action (45). In 1992, Rajfer et al demonstrated that NO induced the production of cGMP leading to cavernosal smooth muscle relaxation and subsequent erection (46). Phosphodiesterases were known to decrease concentrations of cGMP. By 1994, PDE-5 was shown to have its highest concentration in the penis and the reason for sildenafil’s efficacy was discovered (45). The FDA approved sildenafil in March of 1998. Clinical trials to that point had shown that sildenafil could be used on demand, had a low side-effect profile, and was effective in up to 82% of ED patients regardless of etiology (45).
Only gold members can continue reading. Log In or Register to continue

 Detection of Recipient Pretransplant Alloreactivity
Detection of Recipient Pretransplant Alloreactivity
 Surgical Issues in the Transplant Recipient
Surgical Issues in the Transplant Recipient
 Hematologic Complications of Transplantation
Hematologic Complications of Transplantation
 Non-CMV, Non-hepatitis Viral Infections in the Renal Transplant Patient
Non-CMV, Non-hepatitis Viral Infections in the Renal Transplant Patient
 Medical Complications of the Eyes, Nasopharynx, Dentition, Oropharynx, and Hearing in the Kidney Transplant Recipient
Medical Complications of the Eyes, Nasopharynx, Dentition, Oropharynx, and Hearing in the Kidney Transplant Recipient



