Gallbladder cancer is the most common biliary tract cancer. The highest incidence rates occur in Chile, which also has the highest mortality rates. This lethal gastrointestinal cancer has a predilection among adult women and older subjects of both sexes, and also among populations throughout central and Eastern Europe and certain racial groups, such as Native American Indians. Unfortunately, prospects are poor for preventing this form of cancer.
Gallbladder cancer is a rare cancer that was first described more than 2 centuries ago. Individuals with gallbladder cancer usually have no symptoms or signs and deteriorate quickly with the development of metastatic disease. Unfortunately, this gastrointestinal cancer continues to have a poor prognosis because of late diagnosis and few effective treatment options. Gallbladder cancer is an unusual gastrointestinal cancer in that it is much more common among older women than men. The incidence of gallbladder cancer also shows wide geographic and ethnic variations. Understanding the epidemiology of gallbladder cancer has and will continue to provide valuable insights into determining causes and risk factors for gallbladder cancer.
Descriptive epidemiology
Incidence
In describing the incidence of gallbladder cancer, two sources of data have been used. First, the Cancer Incidence in Five Continents, Volume IX (CI5) presents incidence data from populations worldwide. The reference period for this volume was defined as 1998 to 2002. In addition, data was obtained from the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute (NCI), which is a leading source of information on cancer incidence and survival in the United States. SEER currently collects and publishes cancer incidence and survival data from population-based cancer registries covering approximately 26% of the United States population. SEER coverage includes 23% of African Americans, 40% of Hispanics, 42% of American Indians and Alaska Natives, 53% of Asians, and 70% of Hawaiian/Pacific Islanders.
World
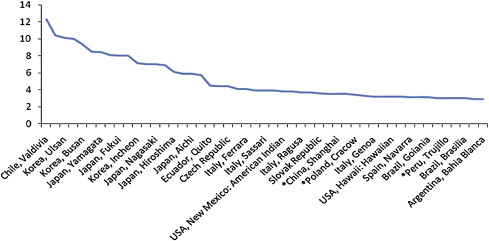
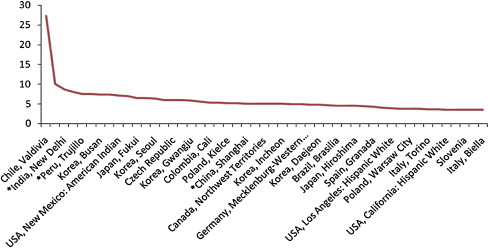
Using data from the CI5 database, the world standardized incidence rates for gallbladder cancer for men ( Fig. 1 ) and women ( Fig. 2 ) was determined. Chile (Valdivia) was found to have the highest incidence of gall bladder cancer among men and women: 12.3 and 27.3 per 100,000 population, respectively (ASW, age-standardized to the world population). Among the top 10 locations around the world, men seem to have very little geographic variation, with regions in Korea and Japan making up most of these. Most of the top 50 locations for gallbladder cancer have an incidence of approximately 3.0 to 4.0 per 100,000. Geographic locations for women however, shows more variation for gallbladder cancer, with regions in India, Peru, Korea, Japan, Columbia, and the United States among the top 10 locations. Among women, incidences of gallbladder cancer among the top 50 locations around the world are higher than those for men, with most between 4.0 and 6.0. The highest incidence rates among women are twice those of men, but incidence rates decline sharply for women and show a steady decline among men.
United States
According to the CI5 data, the highest incidence of gallbladder cancer in the United States occurs among Korean men in Los Angeles and American Indian women in New Mexico (ASW, 5.9 and 7.1, respectively). Among men, American Indians are next in terms of incidence (3.8), with Hawaiians (3.2) in Hawaii, Japanese (2.6) in Los Angeles, and African Americans (2.5) in Connecticut constituting the top five United States locations.
Among the top five United States locations with the highest incidence of gallbladder cancer for women, Hispanic Whites (3.9) from Los Angeles were second, followed by Koreans (3.6) in Los Angeles, Hispanic Whites (3.5) from California, and Hispanic Whites from San Francisco (3.3) . The high incidence of gallbladder cancer among non-White ethnic groups suggests that either genetic or environment factors are responsible for these high rates.
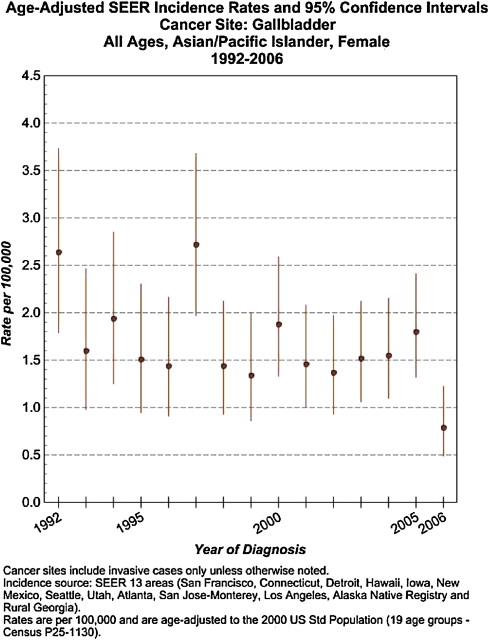
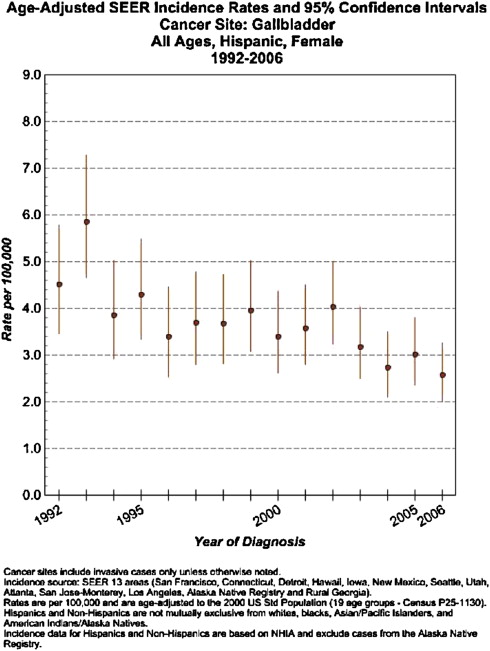
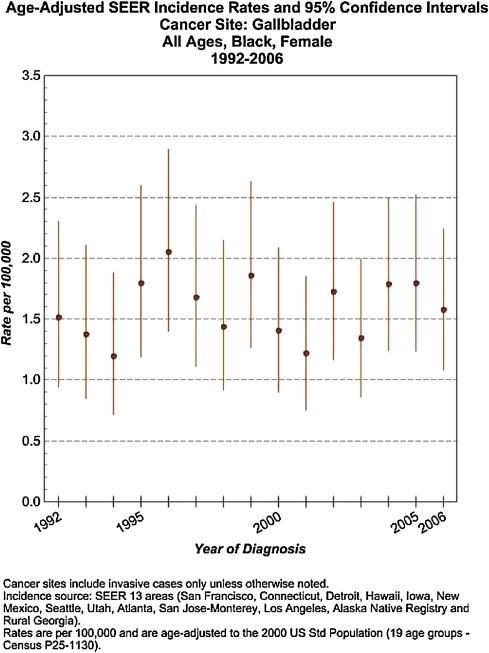
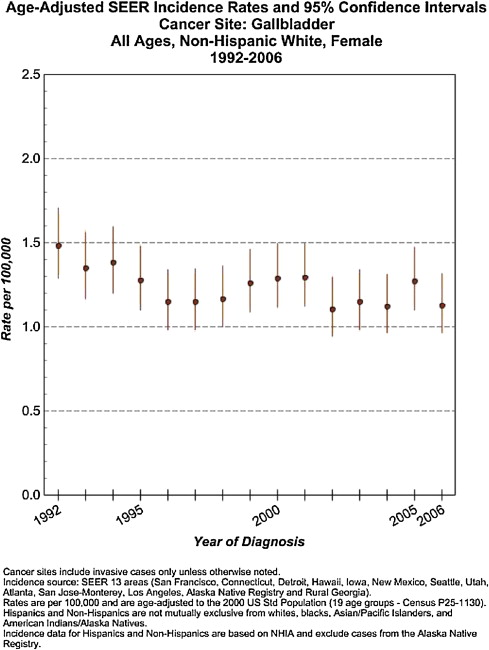
Data from the United States ( Figs. 3–6 ) show changes in incidence over time for women (1992–2006), with Asian/Pacific Islanders showing a gradual decline in gallbladder cancer incidence from 2.7 in 1992 to 0.7 in 2006 (see Fig. 3 ). Hispanics also showed a decreased incidence from 4.5 in 1992 to 2.5 in 2006 (see Fig. 4 ). African Americans showed no real change in incidence over this 15-year period (see Fig. 5 ), which is similar to non-Hispanic White women, who show a very slight decrease during this timeframe (see Fig. 6 ).
Mortality
Worldwide data suggest that Mapuche Indians in Chile and Hispanics have the highest mortality, with North American Indians and Mexican Americans following closely behind. This finding is believed to be caused partly by the lack of medical care available in certain geographic locations.
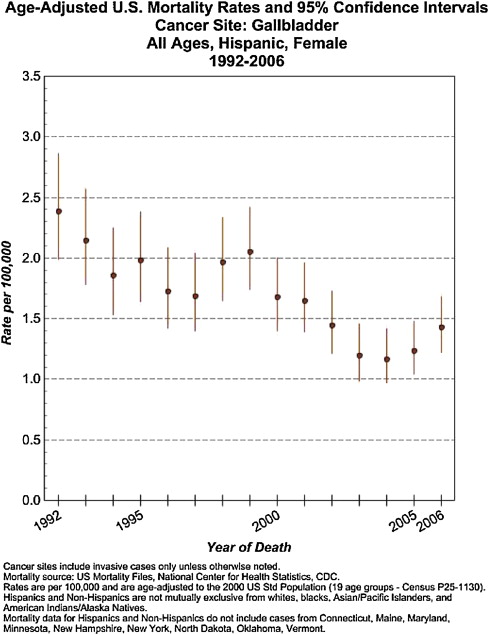
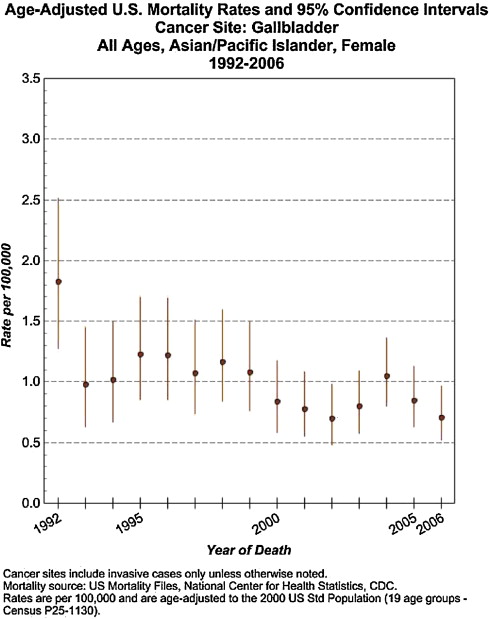
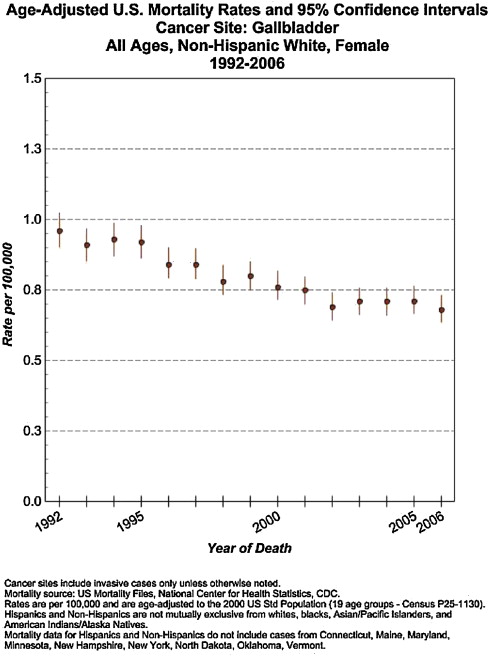
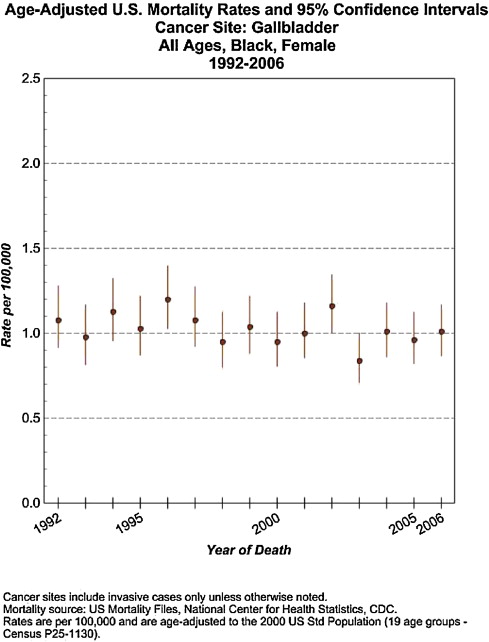
In the United States, SEER mortality data between 1992 and 2006 suggest that the mortality rates for gallbladder cancer are decreasing for some ethnic groups. This decline can be seen among Hispanics ( Fig. 7 ) and Asian/Pacific Islanders ( Fig. 8 ), whereas no change has occurred for African Americans or non-Hispanic Whites ( Figs. 9 and 10 ).
Geographic Variation
Currently, the geographic distribution of gallbladder cancer is not well described. A study on the descriptive epidemiologic trends of gallbladder cancer among 25 European countries between 1965 to 1989 reported the highest mortality rates in Hungary (3.9/100,000 men; 7.4/100,000 women), with high rates also in Germany, Austria, Czechoslovakia, Hungary, and Poland. During the 25-year period assessed, mortality rates were found to have increased in Czechoslovakia and Hungary but were stable in Poland and declined in Austria and Germany. The lowest mortality rates were reported in Belgium, France, Britain, Ireland, Norway, Bulgaria, and Mediterranean countries. Trends among this group found that over the 25-year period, mortality rates declined in Bulgaria and Great Britain but increased in all other countries.
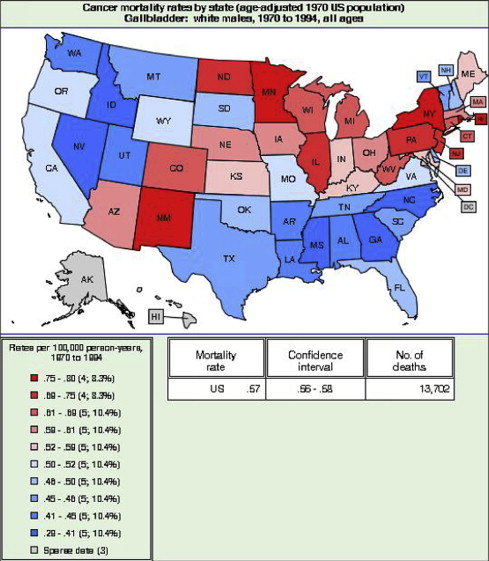
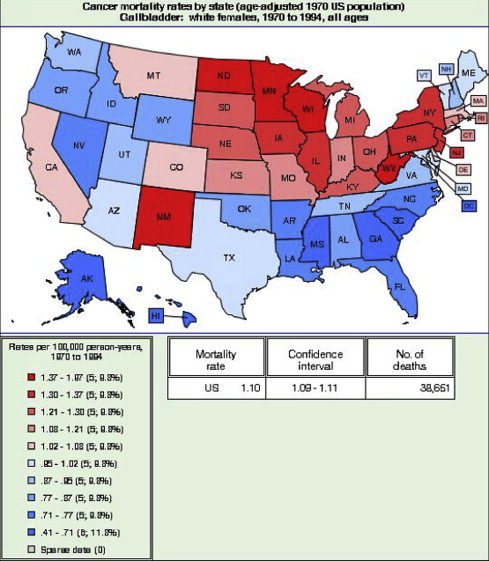
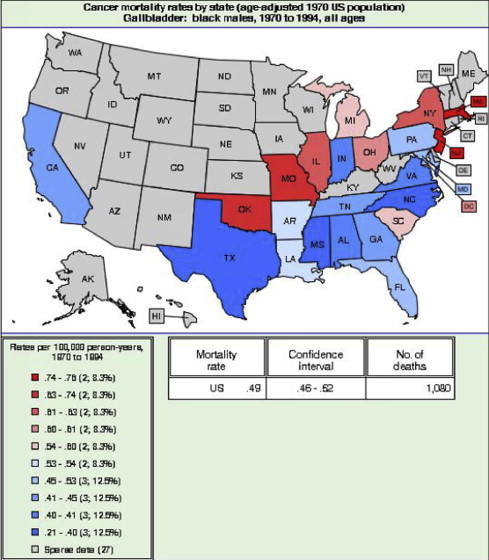
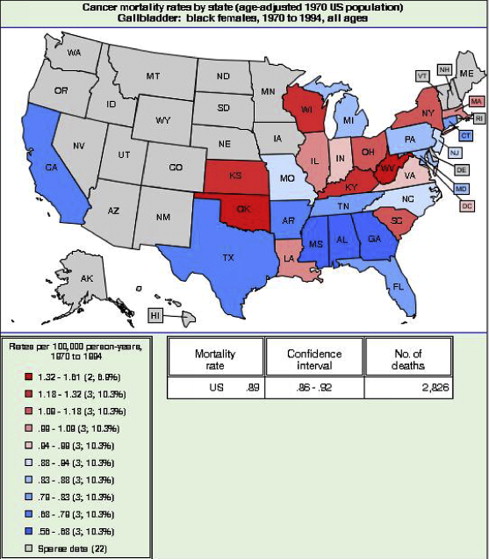
In terms of geographic location in the United States, data from the National Cancer Institute (NCI) between 1970 and 1994 highlight states with high mortality for gallbladder cancer. Among White men, the highest mortality rates occurred in New Mexico, Arizona, Minnesota, North Dakota, Ohio, West Virginia, Maine, and Rhode Island ( Figs. 11 and 12 ). African American had very few high mortality states in during this period, with these only consisting of Oklahoma, Missouri, Massachusetts, and New Jersey ( Fig. 13 ). The highest mortality rates for African American women were seen in Oklahoma, Kansas, Wisconsin, Kentucky, South Carolina, and West Virginia. ( Fig. 14 ).
Another recent study reported that most countries in Europe, Canada, the United States, and the United Kingdom show a decline in gallbladder cancer–associated mortality for both genders. However, increases in mortality among men were found for Iceland, Costa Rica, and Korea. The variation seen in Europe and the United States could reflect the movement of certain populations, International Classification of Diseases coding for gallbladder cancer, changes in diet, or increases in rates of obesity, or that these locations do not offer sufficient diagnostic modalities for individuals with gallbladder cancer or screen high-risk populations within these states.
Risk factors
Traditionally, risk factors for the development of gallbladder cancer have essentially been chronic cholelithiasis and female gender. However, other factors also promote the development of gallbladder cancer. An important risk factor seems to be infection, with studies supporting the relationship with Salmonella typhi . The continual discovery of new organisms presents new possibilities for elucidating important and potentially treatable risk factors.
Age
The incidence of gallbladder cancer increases with age, with the highest incidence usually found in individuals older than 65 years. However, a recent analysis of the SEER database between 1973 to 2002 found a substantial decrease has occurred in the incidence of gallbladder cancer among individuals older than 50 years, and actually reported an increased incidence of gallbladder cancer in younger age groups (<50 years).
Gender
It has long been known that women are more likely to develop gallbladder cancer, with odds ratios suggesting an increased risk ranging between 2 and 8 times that of men. Gallbladder disease has always been associated with the four F s: (1) fat (overweight); (2) age older than 40 years; (3) female gender; and (4) fertile. These risk factors certainly increase a woman’s chance of developing gallbladder disease, but other factors also contribute to the development of gallbladder cancer.
Gallbladder Disease
Gallstone disease is an important risk factor for the development of gallbladder cancer; however, not all individuals with gallstones will develop gallbladder cancer. Moreover, having a history of benign gallbladder diseases increases the risk for developing gallbladder cancer, although some studies do not support this statement ( Table 1 ). Most case-control studies strongly suggest a relationship, whereas cohort studies also support a link but with less strength.
| Study | Participants | Relative Risk (95% CI) | Adjustment |
|---|---|---|---|
| History of benign gallbladder diseases a | |||
| Cohort studies b | |||
| Maringhini et al, 1987 (USA) | 2.8 (0.9–6.6) | Age and sex | |
| Men | 8.3 (1.0–30.0) c | Age and sex | |
| Women | 2.0 (0.4–5.7) c | Age and sex | |
| Chow et al, 1999 (Denmark) | 3.6 (2.6–4.9) | Age and sex | |
| Yagyu et al, 2004 (Japan) | Men | 1.2 (0.3–4.7) | Age |
| Women | 1.1 (0.4–2.9) | Age | |
| Case-control studies d | |||
| Lowenfels et al, 1985 (USA) | Non-Indians | 4.4 (2.6–7.3) | Age, sex, center, alcohol, smoking, education, and response status |
| Indians | 20.9 (8.1–54.0) | Age, sex, center, alcohol, smoking, education, and response status | |
| Nervi et al, 1988 (Chile) | 7.0 (5.9–8.3) | Age, sex, country | |
| WHO, 1989 e | 2.3 (1.2–4.4) | None reported | |
| Kato et al, 1989 (Japan) | 34.4 (4.51–266.0) | None reported | |
| Zatonski et al, 1997 f | 4.4 (2.6–7.5) | Age and sex | |
| Okamoto et al, 1999 (Japan) | 10.8 (4.1–28.4) g | ||
| Khan et al, 1999 (USA) | 26.6 (7.0–101.4) | Sex, age, ethnicity, smoking, and socioeconomic status | |
| Women | 28.9 (4.7–173.0) c | Age, ethnicity, socioeconomic status, hysterectomy, menopause, parity, diabetes, and smoking | |
| Family history of benign gallbladder diseases | |||
| Case-control studies h | |||
| Kato et al, 1989 (Japan) | 3.0 (1.3–6.5) | None reported | |
| Strom et al, 1995 (Bolivia, Mexico) | 3.6 (1.3–11.4) | Age, sex, and hospital | |
| Family history of gallbladder cancer i | |||
| Cohort studies j | |||
| Goldgar et al, 1994 (USA) | First-degree relatives | 2.1 (0.2–6.1) | Age at diagnosis |
| Hemminki et al, 2003 (Sweden) | Parents | 5.1 (2.4–9.3) | Age, sex, region, period, and socioeconomic status |
| Offspring | 4.1 (2.0–7.6) c | Age, sex, region, period, and socioeconomic status | |
| Case-control studies | |||
| Fernandez et al, 1994 (Italy) | First degree relatives | 13.9 (1.2–163.9) | Age, sex, residence, and education |
a Summary relative risk for all studies was 4.9 (95% CI, 3.3–7.4) and heterogeneity test between studies was χ26=57.361
χ 6 2 = 57.361
; P <.001.
b Summary relative risk for cohort studies was 2.2 (95% CI, 1.2–4.2) and heterogeneity test between studies was χ23=6.918
χ 3 2 = 6.918
; P = .075.
c Not included in the summary estimates.
d Summary relative risk for case-control studies was 7.1 (95% CI, 4.5–11.2) and heterogeneity test between studies was χ27=28.540
χ 7 2 = 28.540
; P <.001.
e Chile, China, Colombia, Israel, Kenya, Mexico.
f Australia, Canada, Netherlands, Poland.
g Estimated from available data.
h Summary relative risk for case-control studies was 3.2 (95% CI, 1.7–6.1) and heterogeneity test between studies was χ21=0.007
χ 1 2 = 0.007
; P = .791.
i Summary relative risk for all studies was 4.8 (95% CI, 2.6–8.9) and heterogeneity test between studies was χ22=1.647
χ 2 2 = 1.647
; P = .439.
j Summary relative risk for cohort studies was 4.5 (95% CI, 2.4–8.5) and heterogeneity test between studies was χ22=0.895
χ 2 2 = 0.895
; P = .344.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


