CHAPTER 17 Endoscopic component separation
Step 1. Surgical anatomy
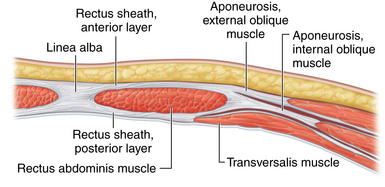
♦ The rectus abdominis muscle is a paired muscle running vertically from the costal margin to the inguinal ligament. It is separated in the midline by the linea alba. Along its lateral borders are the fused aponeuroses of the external oblique, internal oblique, and transversus abdominis muscles.
♦ Abdominal wall hernias often occur in the midline at the linea alba. Often, a great distance separates the rectus muscle bellies. During repair, there may be excessive tension when the muscles are pulled together to re-create the midline. One technique that can be helpful is to release the rectus abdominis muscle from some of its lateral attachments to pull it medially.
♦ To separate the rectus abdominis muscle from the external oblique muscle, an incision needs to be lateral to the fused aponeuroses of the external and internal oblique muscles. This will allow the internal oblique/transversus abdominis/rectus abdominis unit to “release” medially. Full separation of the flimsy fibroareolar connective tissue between the oblique muscles will maximize mobilization of the rectus muscle bellies medially (Figure 17-1).
Step 2. Preoperative considerations
Patient preparation
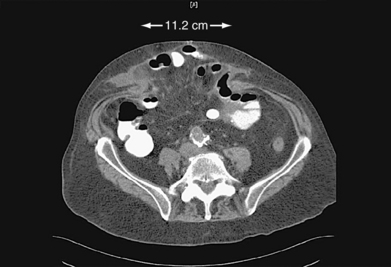
♦ Endoscopic component separation (ECS) is most useful for patients with midline defects of more than 5 to 8 cm in width as measured between the medial borders of the rectus muscle bellies (Figure 17-2).
♦ Symptoms associated with large defects that can be improved with component separation include a large abdominal wall deformity, difficulty leaning forward, difficulty fitting clothes, and discomfort related to pressure pushing the skin outward. Less clearly associated symptoms include inability to carry out activities of daily living or work, skin ulceration, and difficulties with an ostomy appliance if present.
♦ Component separation can be incorporated with open, laparoscopic, or laparoscopic-assisted hernia repair. Patient selection for each approach is based on the specific clinical characteristics, most of which can be determined preoperatively with a physical examination and computed tomography (CT). Open and laparoscopic-assisted approaches have the advantage of suturing the midline together with more accuracy and strength, compared to laparoscopic techniques.
 An open approach is typically planned for those requiring scar revision (because of ulcers, thin skin, previous skin graft, or unsightly scar) or explantation of a large prosthetic.
An open approach is typically planned for those requiring scar revision (because of ulcers, thin skin, previous skin graft, or unsightly scar) or explantation of a large prosthetic.

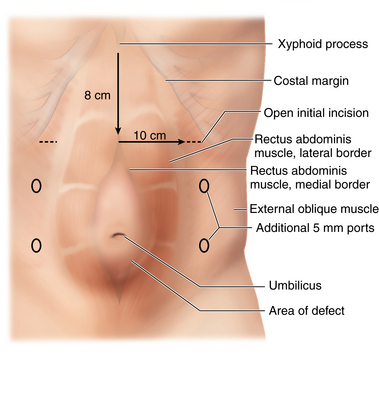
♦ Preoperative CT is useful for operative planning if considering a laparoscopic or laparoscopic-assisted approach. The exact dimensions of the defect can be ascertained, along with the calculated location of the lateral border of the rectus abdominis muscle. The latter measurement is particularly important if performing ECS as the initial portion of the operation (Figure 17-3).
♦ Prior abdominal access in the vicinity of the rectus and oblique muscles pose potential difficulty because of adhesions between fascial planes. Examples include open appendectomy or laterally based ostomy sites.
Equipment and instrumentation
♦ A standard handheld Bovie is adequate for dissection of the space between the oblique muscles. Deep thin retractors such as S-retractors are also useful during this part of the procedure.
♦ A dissecting balloon (OMSPDB 1000 Covidien, Mansfield, Massachusetts) facilitates the creation of the space between the oblique muscles prior to insufflation (Figure 17-4).
♦ A port with a balloon at the distal end (OMST10BT Covidien, Mansfield, Massachusetts) or a valveless port (AirSeal; Surgiquest, Orange, CT) helps prevent leakage during insufflation. There is limited space between the muscles. This port can be pulled all the way back to the tip, and the balloon tip prevents inadvertent removal of the port. This gives the best view of the small space (Figure 17-5).


Anesthesia
♦ Regardless of the exact operative approach, general anesthesia is required. Consideration should also be given for epidural catheter placement to assist with postoperative pain management.
♦ Antibiotics: routine prophylactic antibiotics to cover gram-positive organisms should be administered prior to surgery. In longer cases, antibiotic redosing may be necessary. Postoperative antibiotics are not routinely required.
♦ A three-way bladder catheter is useful to avoid injury to the urinary bladder when dissecting in the pelvis. The bladder is filled with approximately 300 cc of saline and the catheter clamped. Once this portion of the dissection is complete, the clamp is removed.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


