Endometriosis and Endosalpingiosis
Colonic involvement occurs in 3% to 34% of women with endometriosis. Patients range in age from 28 to 56 years (609). Recurrent, crampy, mild abdominal pain is the most common presenting symptom. Patients may also present with nausea, vomiting, diarrhea, constipation, small-caliber stools, fever, anorexia, weight loss, hematochezia, a mass, intestinal obstruction, and infertility. Because of the predominantly serosal and subserosal location of the tissue, rectal bleeding is infrequent. An episodic and cyclic nature of the intestinal symptoms just prior to menstruation clinically suggests the diagnosis. However, symptoms coincide with menstruation in <50% of cases (610). Extensive and deep involvement of the intestinal wall (Fig. 13.174) or the inflammatory adhesions produced by resolution of recurrent episodes of bleeding may lead to intestinal obstruction,
volvulus, or intussusception. Rarely, the disorder presents as an acute abdomen. Terminal ileal disease mimics malignancy, strictures from previous radiotherapy, CD, ischemia, and infections such as Yersinia and tuberculosis (Fig. 13.175).
volvulus, or intussusception. Rarely, the disorder presents as an acute abdomen. Terminal ileal disease mimics malignancy, strictures from previous radiotherapy, CD, ischemia, and infections such as Yersinia and tuberculosis (Fig. 13.175).
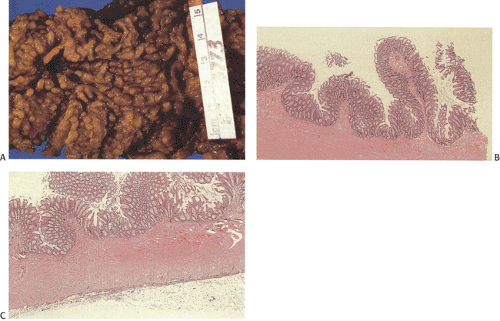 FIG. 13.173. Reactive fibromuscular proliferations. A through C are from the same specimen. A: Grossly innumerable short, stubby, mucosal projections are present. B: These consist of mucosal elevations by a proliferation of smooth muscle mixed with vessels and nerves. There is complete loss of the demarcation between the muscularis mucosae, submucosa, and muscularis propria. C: Higher magnification showing the obliteration of these normal landmarks. |
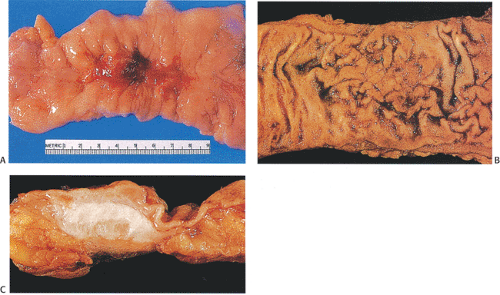 FIG. 13.174. Endometriosis. A: Gross appearance of the fresh specimen with prominent mucosal puckering and localized hemorrhage. B: Fixed specimen with submucosal endometriosis. C: Cross section through the bowel wall of previous specimen demonstrates prominent mucosal fibrosis. |
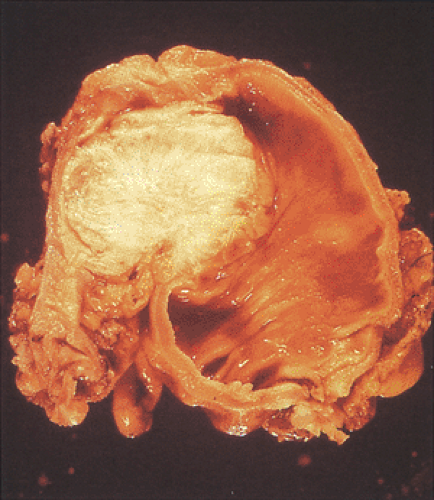 FIG. 13.175. Endometriosis presenting grossly as a cecal carcinoma. |
Intestinal endometriosis commonly affects those parts of the bowel that lie in proximity to genital organs. The sigmoid is the most commonly affected portion of the large bowel, followed by the rectum (611), with these two sites accounting for 70% of cases. The lesions present grossly as intramural masses of strictures or stenosis, polyps, or submucosal masses simulating a carcinoma. The serosal surface is often puckered secondary to extensive subserosal fibrosis. This may lead to secondary stricture formation. The presence of a hard annular growth that usually spares the mucosa may simulate a carcinoma. Adhesions to adjacent structures may develop. Cut sections of the bowel wall may disclose the presence of small intramural tarry or chocolate cysts.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


