Fig. 6.1
An illustration of how traditional approaches to pelvic floor dysfunctions have been segmented according to disciplines and pelvic compartments
There is a common agreement that many problems or challenges in society cannot be solved appropriately without an interdisciplinary, or at least a multidisciplinary approach [24]. This is also most likely true in medicine. Complex patient problems have multiple facets, each of a particular concern to one medical speciality or health care discipline. In other words, on one hand a number of challenges will most likely be insufficiently solved by one speciality or discipline only. On the other hand, a number of complex problems or challenges will not be satisfactory solved without the presence of the relatively narrow and specialized competence each medical speciality or health care discipline provide.
Multidisciplinary approach is never the less a challenge where hope often tends to triumph over experience, and this can easily stop the process of establishing a successful team. The important question is: why is it so?
The word discipline originates from the Latin word disciplus, which means obedient pupil and follower. The characteristics of a single speciality or discipline is specific structure and system of knowledge, language, and culture, reproduced by training [25], and disciplined thinking explicitly or implicitly “ . . . omits or ignores a great many other possible causes and explanations—it would not be disciplined if it did not” [26]. This is also true for medical specialities, which is not just part of a particular medical subject matter, but also a system of rules, reproduced by schooling, training and practice. Medical specialities are evolved by many factors but also by:
Developing language in form of expressions, theories, and concepts belonging to their field
Identifying and isolating the patients main problem
Identifying the main cause and effect relationship
Multidisciplinary teamwork is defined as: coupling of contributors from several disciplines to enlighten a common challenge. The different disciplines are working next to each other and there is no disciplinary integration, but the different contributors can inspire and develop the single disciplines contributors [25].
In addition to contribution from different disciplines there are real scientific integrations of the different contributions, theoretically and/or methodologically in interdisciplinary teamwork [25, 26]. In other words, multidisciplinary and especially interdisciplinary teamwork possesses a challenge since it somewhat contradicts the construct of a discipline. Optimal care of pelvic floor dysfunction after treatment of pelvic cancer will sometimes require a multidisciplinary approach, whereas other times the superb appropriate approach is interdisciplinary.
Due to the challenging nature of multi/interdisciplinary work it is necessary with some core structures for the team to work within to establish a good functioning pelvic floor team. This requires steady coordination and focus from someone having a principal responsibility to see the processes of the teambuilding through and to follow-up thereafter.
The Team
Who should be part of the team? In a team caring for patients with pelvic floor dysfunctions there should ideally be a gynecologist, urologist, colorectal surgeon, specialized nurse physiotherapist, radiologist and psychologist involved. However, sometimes there might not be enough resources to establish such a grand team. A vital success criterion, regardless of how many disciplines there is access to, is the motivation of each team member. A team is better off with four motivated members that have acknowledged and are willing to cooperate within the concept of multi/interdisciplinary work, instead of nine unmotivated uncooperative members.
Patient Care Lines
It is essential to establish consensus of the patient care lines that includes all steps to the final clinical audit. This is the frame of the clinical care production, i.e. investigations and treatments, involving the multi/interdisciplinary team. It is however important to understand that it is not only a “check-mark” system. While the system should ensure that investigation and/or treatment paths are followed, the multi/interdisciplinary thinking should also identify patients that show signs indicating that a more tailored and personalized path is necessary (Fig. 6.2).
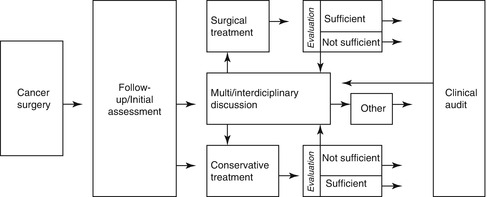
Fig. 6.2
An example of patient care lines with a multi/interdisciplinary approach for patients after cancer surgery
Multi/Interdisciplinary Meetings
This is the arena for which the patients with complicated problems are discussed by the team. There are several purposes of multi/interdisciplinary meetings. First and foremost it is to achieve a common consensus based on the insight and knowledge generated from the whole group. Second, it is a learning arena for the team, expanding their knowledge by gaining knowledge from the other disciplines, and thirdly, this is where the process is audited. When the patient is discharged, the team should be presented an overview of the decisions, the investigations and treatments and the final outcome. It is advisable to have one person coordinating the meetings. The coordinator is responsible for:
Calling the meeting with the appropriate team members (sometimes additional disciplines than the core team are needed)
Preparing the cases for discussion
Ensure that the patients get appointments according to the decided plan
Follow-up with a written discharge plan when the patient is finished
Present the final result to the group
Common Language, Evaluation: And Scoring-Tools
Each discipline usually has its own sets of tools evaluating the relatively narrow field of the discipline. To create a functional environment where clinical findings can be shared and evaluated by all members of the team, it has to be consensus of what type of scoring/evaluation tools to use for sharing, evaluating and comparing results within the group. If a system for clinical audit is established it is advisable to use validated scorings tool so that the data can be used for publications as well. Locally developed or not validated systems like incontinence diaries may be used additionally. Table 6.1 [27–36] shows an overview of relevant scoring tools.
Table 6.1
Some relevant scoring tools for assessment of pelvic dysfunctions
Scoring tool | Reference |
|---|---|
Anal incontinence | |
St. Mark’s score | Vaizey et al. [27] |
Wexner incontinence score | Jorge and Wexner [28] |
ICIQ-B | Cotterill et al. [29] |
Low anterior resection syndrome | |
LARS-score | Emmertsen and Laurberg [30] |
Constipation | |
KESS | Knowles et al. [31] |
Wexner constipation score | Agachan et al. [32] |
Obstructed defecation | |
Obstructed defecation syndrome score | Renzi et al. [33] |
Stress urinary incontinence | |
ICIQ_UI_SF | Abrams et al. [34] |
Roos screening test | Roos and Thakar [35] |
Sexual dysfunction (men) | |
IIEF-5 | Rosen et al. [36] |
Pain | |
VAS-scale | |
Defining Responsibilities for Each Member of the Team
In all type of teamwork, there is a potential risk of destructive group dynamics: some not doing their share of work, some doing a vast amount of work, some that are very visible and others that are more or less invisible. These are dynamics that might cause a dysfunctional group. All members should be aware of their responsibility within the team, and the team manager should be able to address these issues and ensure a “healthy” group dynamic.
Creating Organizational Changes Where It Is Necessary and Possible
To allow a multi/interdisciplinary practice there might be necessary with organizational changes. As for example, if the patient is scheduled to see both physiotherapist and a nutritionist, the system should allow the patient to see them both in 1 day. To organize relevant outpatient clinics on the same day will also allow team members to naturally work closely in the clinical setting.
Clinical Audit
System for clinical audit is essential to evaluate the work and the processes. It is however a challenge to create a system that are crossing disciplines since the whole hospital organization is more often than not based on disciplines. Thus patient journal systems, management, traditional patient flow and care lines follow these rather rigid and straight-line structures. Because of this it is even more important to strive toward a good audit system to evaluate the result and resource used.
In addition, it is also important to acknowledge the importance of social skills in such work:
Openness, trust and mutual respect is perhaps easier said than done but essential when highly skilled people shall collaborate and give good results
There is not one discipline “owning” the problem, nor the solution.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







