Recent progress of the data processing applied to ultrasonographic (US) examination has made it possible to develop new software. The US workstation of the last generation thus incorporated in their center a computer allowing a precise treatment of the US image. This advancement has made it possible to work out new images such as 3-dimensional (3D) US, contrast harmonic US associated with the intravenous injection of contrast agents, and even more recently, elastography. These techniques, quite elaborate in percutaneous US at present, are to be adapted and evaluated with endoscopic US (EUS). The contribution of contrast agents of US to pancreatic EUS and then 3D EUS are successively approached in this article.
Recent progress of the data processing applied to ultrasonographic (US) examination has made it possible to develop new software. The US workstation of the last generation thus incorporated in their center a computer allowing a precise treatment of the US image. This advancement has made it possible to work out new images such as 3-dimensional (3D) US, contrast harmonic US associated with the intravenous (IV) injection of contrast agents, and more recently, elastography. These techniques, quite elaborate in percutaneous US at present, are to be adapted and evaluated with endoscopic US (EUS).
The contribution of the contrast agents of US to pancreatic EUS and then 3D EUS are successively approached in this article.
Contrast-enhanced EUS
Among several technologies, EUS has been widely used to diagnose pancreatic, lymph node, and gastrointestinal (GI) tumors because EUS is superior to any other modality with respect to spatial resolution. However, EUS has limitations in evaluating vascularity by contrast US when the color Doppler or power Doppler mode is used. Contrast-enhanced power Doppler US is accompanied by artifacts, for example, blooming, so that the width of a blood vessel visualized by the power Doppler mode is magnified and wider than that visualized by fundamental B-mode imaging. Contrast harmonic imaging by IV infusion of Levovist (SHU508 A), an air-filled microbubble with an outer shell composed of 99.9% galactose and 0.1% palmitic acid, has allowed the observation of the vasculature of the abdominal organs on transabdominal US. If the US equipment receives harmonic components that are integer multiples of the fundamental frequency, then the harmonic content derived from microbubbles is higher than that from tissues. Contrast harmonic imaging detects signals from microbubbles and filters the signals that originate from tissue by selectively detecting the harmonic components. This technology can detect signals from microbubbles in vessels with a very slow flow without Doppler-related artifacts and is used to characterize tumor vascularity in liver, pancreas, gallbladder, and GI tract during transabdominal US. Until recently, there was no contrast harmonic imaging available for EUS examination because the transducer for current echoendoscopes is of a limited frequency bandwidth and is too small to produce enough acoustic power for contrast harmonic imaging when using Levovist. Second-generation US contrast agents (UCAs), for example, SonoVue, produce harmonic signals at lower acoustic powers and, therefore, are suitable for EUS at low acoustic powers.
General Considerations
UCAs, in conjunction with contrast-specific imaging, are increasingly accepted in clinical use for diagnostic imaging and postinterventional workup in several organs. To those not closely involved in the field, the rapid advances in technology and techniques can be difficult to follow. In March 2003, at the European Federation of Societies for Ultrasound (EUROSON) Congress in Copenhagen, it was agreed that it would be useful to produce a document providing a description of essential technical requirements, proposed investigator qualifications, suggested study procedures and steps, guidance on image interpretation, and recommended and established clinical indications and safety considerations.
The development of UCAs, which perform as blood pool tracers, has overcome the limitations of conventional B-mode and color Doppler or power Doppler US and enable the display of parenchymal microvasculature. Depending on the contrast agent and the mode of US, the dynamic lesion enhancement pattern is visualized during intermittent or continuous imaging. Enhancement patterns are described during subsequent vascular phases (eg, arterial, portal venous, and late phases for liver lesions), similar to contrast-enhanced computed tomography (CECT) and/or contrast-enhanced magnetic resonance imaging (CEMRI). Contrast-enhanced US (CEUS) and CECT or CEMRI are not equivalent because UCAs have different pharmacokinetics and are confined to the intravascular space, whereas most of the currently approved contrast agents for CT and MRI are rapidly cleared from the blood pool into the extracellular space.
An inherent advantage of CEUS is the possibility to assess the contrast enhancement patterns in real time with a substantially higher temporal resolution than other imaging modalities and without the need to predefine time points of scans or perform bolus tracking. Furthermore, administration of UCAs can be repeated because of the excellent patient tolerance to them.
In addition to IV use, intracavity applications of the UCAs, such as intravesical administration, can be performed.
Studies on Ultrasound Contrast Agents are subject to the same limitations as other types of US studies. As a general rule, if the baseline result of US is very suboptimal, CEUS may be disappointing.
Commercially Available UCAs in Europe
At present, 4 transpulmonary UCAs are approved and marketed within European Countries:
- 1.
Levovist (air filled, with galactose and palmitic acid as a surfactant; introduced in 1996). Main indications include vesicoureteric reflux and cardiac, abdominal, and transcranial applications.
- 2.
Optison (octafluoropropane (perflutren) with an albumin shell; introduced in 1998). Sole indication to date is in cardiac applications.
- 3.
SonoVue (sulfur hexafluoride with a phospholipid shell; introduced in 2001). Approved indications are cardiac (endocardial border delineation), macrovascular (cerebral and peripheral arteries, portal vein), and microvascular (characterization of focal lesions in liver, pancreas, and breast).
- 4.
Luminity (octafluoropropane perflutren with a lipid shell; introduced in 2006). Sole indication to date is in cardiac applications.
There are other UCAs that are approved outside Europe or under investigation.
The UCAs that are used at present in diagnostic US are characterized by a microbubble structure consisting of gas bubbles stabilized by a shell. UCAs act as blood pool agents. They strongly increase the US backscatter and therefore are useful in the enhancement of echogenicity for the assessment of blood flow. Although conventional US can detect high concentrations of microbubbles, in practice, their assessment usually requires contrast-specific imaging modes.
Contrast-specific US modes are generally based on the cancellation and/or separation of linear US signals from tissue and use of the nonlinear response from microbubbles.
Nonlinear response from microbubbles is based on 2 different mechanisms:
- 1.
Nonlinear response from microbubble oscillations at low acoustic pressure, chosen to minimize disruption of the microbubbles.
- 2.
High-energy, broadband, nonlinear response arising from microbubble disruption. Nonlinear harmonic US signals may also arise in tissues because of a distortion of the sound wave during its propagation through the tissue. The extent of this harmonic response from the tissue at a given frequency increases with the acoustic pressure, which is proportional to the mechanical index (MI).
Low-solubility gas UCAs (eg, SonoVue, Optison, Luminity) are characterized by the combination of improved stability with favorable resonance behavior at low acoustic pressure. This combination allows minimally disruptive contrast-specific imaging at low MI and enables effective investigations over several minutes with the visualization of the dynamic enhancement pattern in real time. Low-MI techniques, furthermore, lead to effective tissue-signal suppression because the nonlinear response from the tissue is minimal when low acoustic pressures are used. US imaging with air-filled microbubbles (eg, Levovist) at high pressure depends on microbubble disruption, which is a significant limitation for real-time imaging.
Pancreatic EUS and UCAs
Diagnosis between adenocarcinomas and nodular chronic pancreatitis is problematic. All methods of diagnosis are limited. Histology is the standard diagnosis, but even biopsy can be difficult because cancers can produce a marked fibrotic reaction or necrosis and give false results. When there is a stenosis of the main pancreatic duct, the sensitivity and specificity of endoscopic retrograde cholangiopancreatography (ERCP) are 85% and 66%, respectively. Magnetic resonance cholangiopancreatography (MRCP) has a similar sensitivity and specificity as that of ERCP for detecting pancreatic cancer or chronic pancreatitis.
Nevertheless, sensitivity is yet to be perfectible, and MRCP gives a correct differentiation between malignant and benign lesions in 58% of the cases. MRCP remains as an expensive procedure, is time-consuming, and is available only in a few centers.
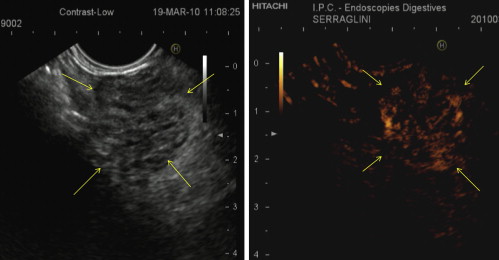
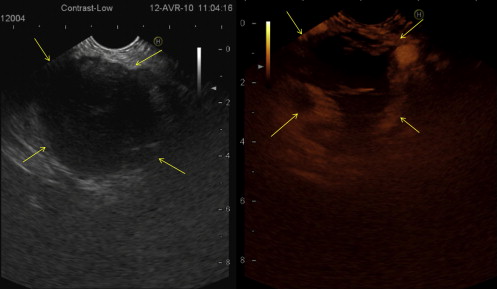
There are few studies about contrast-enhanced EUS (CE-EUS). Bhutani and colleagues evaluated the utility of Levovist and concluded that it could potentially improve the accuracy of EUS in the diagnosis of malignant vascular invasion, detection of occult pancreatic neoplasms, and diagnosis of vascular thrombosis. Subsequently, Hirooka and colleagues studied the presence or absence of enhancement of different lesions with Albunex in 37 patients. An enhancement of the lesion was observed in 100% of the patients with islet cell tumor ( Fig. 1 ), 80% with intraductal papillary mucinous tumor (IPMT), and 75% with chronic pancreatitis and no enhancement effect was observed in the patients with carcinoma ( Fig. 2 ). All patients underwent angiography, and comparison between images of CE-EUS and angiography showed similar results, except for 3 patients (2 with IPMT and 1 with chronic pancreatitis) in whom angiograms showed hypovascularity, but enhancement effect was observed on EUS images. Becker and colleagues evaluated 23 patients with another contrast agent (FS 069 Optison) and evaluated CE-EUS as a method of differentiating inflammation and carcinoma based on perfusion characteristics. Markedly hyperperfused lesions were considered as inflammatory pseudotumors, whereas lesions that were hypoperfused than the surrounding tissue were considered as carcinomas. For the differentiation of pancreatic carcinoma and inflammatory changes the sensitivity was 94%, specificity 100%, positive predictive value (PPV) 100%, and negative predictive value (NPV) 88%. These results are similar to that obtained by Giovannini (sensitivity 90.9%, specificity 88.8%, PPV 88.2%, and NPV 91.4%). Giovannini also studied hyperechoic lesions (supposed not to be a pancreatic adenocarcinoma), and the sensitivity was 88.8%, specificity 90.9%, PPV 91.4%, and NPV 88.2%. In future, CE-EUS could provide a direct and reliable result (malignant or not) without the need to wait several days for histologic findings. Perhaps, CE-EUS could also save time and money in limiting the use of expensive EUS needles. CE-EUS could be an interesting complement to EUS fine-needle aspiration (EUS-FNA) concerning diagnostic accuracy. The sensitivity and diagnostic accuracy of EUS-FNA are 75% to 92% and 79% to 92%, respectively. First reason, EUS-FNA is not realizable in 6% to 9% of cases owing to vessel interpositions, duodenal stenosis, and tumor hardness, particularly in chronic pancreatitis. Sensitivity of EUS-FNA is limited by uninterpretable material (bleeding or noncellular samples), ranging from 9% to 19% of cases. Totally, the lack of sensitivity of EUS-FNA ranges from 8% to 25% of cases. In the study by Hocke and colleagues, sensitivity and diagnostic accuracy of this technique were comparable to cytopathologic results guided by EUS (sensitivity 90.9%, specificity 88.8%, PPV 88.2%, and NPV 91.4%). From a more general point of view, 97% of hypoechoic lesions were malignant tumors (30 adenocarcinomas, 1 endocrine tumor, 1 pancreatic lymphoma, and 1 pancreatic metastasis from colonic cancer). Therefore, CE-EUS could be a reliable and complementary tool for EUS-FNA in the detection and classification of pancreatic lesions when performing EUS-FNA is impossible or biopsy results are uninterpretable. CE-EUS could improve accuracy and allows to propose an appropriate treatment (eg, surgery, follow-up, chemotherapy).
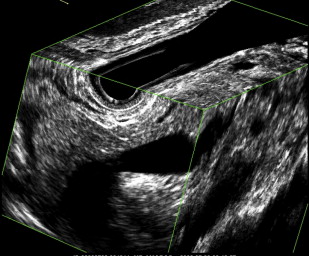
CE-EUS could differentiate a malign tumor from a pseudotumoral nodule ( Fig. 3 ). Chronic pancreatitis is also a limiting factor for diagnosis of pancreatic masses. Several studies have attempted to establish imaging criteria for EUS (without tissue sampling) for differentiating benign inflammatory pseudotumors and tumors. Despite the high resolution of EUS, it does not provide reliable differentiation of benign and malignant lesions of the pancreas. Fritscher-Ravens and colleagues found that the sensitivity of EUS-FNA in patients with a focal pancreatic lesion without chronic pancreatitis was 89%, whereas it was only 54% in patients with chronic pancreatitis. Nevertheless, diagnosis of EUS-FNA influenced clinical management in nearly half of the patients. CE-EUS could also play an important part in the case of lesions occurring within chronic pancreatitis. Indeed, in the study of Hocke and colleagues, adenocarcinoma that developed on chronic pancreatitis was nonenhanced after contrast injection. Conversely, pseudotumoral nodule (benign masses) (91%) in chronic pancreatitis was hypervascularized after SonoVue injection. These results are different and better than studies with CE-EUS. In the study by Takeda and colleagues, 100% of the masses of pseudotumoral pancreatitis had an isoenhanced pattern and it was difficult to differentiate adenocarcinomas from inflammatory pancreatic mass (50% were not well classified).
CE-EUS could be useful in the case of negative results after EUS-FNA. In early studies, NPV of EUS-FNA was around 75%, but most recent studies found NPV to be between 26% and 44%. In the study by Oshikawa and colleagues, the rate of patients with negative results of the first biopsy but with malignant tumor diagnosed a second time with a new puncture or surgery, was 47%.
To conclude, the NPV of pancreatic EUS-FNA is 30% to 33%. Theoretically, a new puncture is mandatory to be sure that it is normal tissue. CE-EUS could avoid this second procedure. With regard to false-negative results with SonoVue, 3 adenocarcinomas were found that presented hyperechoic aspect (contrast-enhancement pattern), 2 of which were poorly differentiated adenocarcinomas and the third was associated with IMPT. This finding suggests that poorly differentiated adenocarcinoma could have different vascularity than well-differentiated adenocarcinoma. These results were similar to studies with CE-EUS. Differences in histologic findings, such as histologic differentiation grade, amount of fibrosis, and obliteration of blood vessels in the tumor, may be associated with differences in enhancement behavior.
Concerning CE-EUS and endocrine tumors, there is only 1 case report using Levovist that seems to be a useful diagnostic method for precise localization of small insulinoma. In the study by Hocke and colleagues, 87.5% (7 of 8) of endocrine tumors had a strong contrast-enhancement pattern, indicating hypervascular lesions. These results were similar to studies with CE-EUS. These vascular images differed from those of almost all pancreatic ductal carcinomas. Thus, differentiation of enhancement pattern on CE-EUS between pancreatic adenocarcinomas and endocrine tumors is useful in the diagnosis of these lesions. In addition, standard EUS is already known to have a great value for localizing endocrine pancreatic tumors because of its excellent capacity to visualize small lesions and tumor vascularization at the same time. Therefore, CE-EUS could increase sensitivity of diagnosis of pancreatic tumors.
Regarding IPMT, in the study by Hocke and colleagues, the only benign tumor was hyperechoic, whereas in malignant IPMT, one was hypoechoic and another was hyperechoic. In the studies on CE-EUS, malignancy could be associated with contrast enhancement. In the study by Sofuni and colleagues, in all 4 patients with IPMT, hypervascularity of the nodules inside the tumors was observed. In the study by Nagase and colleagues, 2 of the 5 IPMTs had solid components within the tumors, and they were positive for enhancement effects. All 5 patients with IPMT underwent surgical resection, and pathologic examination revealed malignancy in the 2 lesions with solid components and positive enhancement. Itoh and colleagues observed that when patients with carcinoma were compared with those with adenoma, the postenhancement intensity was significantly higher in the carcinoma group. CE-EUS could be useful for the differential diagnosis of benign and malignant IPMT. However, the small number of patients with IMPT in each study did not allow conclusions to be made.
Metastatic lesions of the pancreas are rare, between 5% and 10%, but they are an important cause of focal pancreatic lesions. There is only one description of one case of kidney metastasis analyzed by CE-EUS. The study by Giovannini is the first in the literature that describes the enhancement pattern of pancreatic metastasis in CE-EUS. All metastasis except 1 (4 of 5; 80%) showed an echoenhancement pattern, probably proving their hypervascularization. The only nonenhanced pancreatic metastasis was from colonic cancer. CE-EUS could contribute to the differential diagnosis between a primary pancreatic carcinoma and pancreatic metastasis and therefore can have a decisive influence on the selection of appropriate therapeutic strategies (eg, chemotherapy rather than surgery). However, histology remains the standard diagnosis in the differential diagnosis of pancreatic tumors.
CE-EUS in Discrimination Between Benign and Malignant Mediastinal and Abdominal Lymph Nodes
Presence of enlarged mediastinal or abdominal lymph nodes without causing disease is nowadays a clinical issue because of the rapid development of imaging with an increasingly higher resolution of intrathoracic or intra-abdominal structures. At present, CT scanners reliably recognize lymph nodes of 5 to 10 mm in size but do not distinguish between malignant and benign lymph nodes in most cases. EUS has an even higher local resolution, but again, given a distinct visible lymph node, the investigator is frequently not able to assign this node to a malignancy, whether or not a malignant tumor is already known. There are several US features such as size, round shape, hypoechoic appearance, missing hilus sign, and clear borders, which cumulatively make a malignant lymph node most likely. But on the one hand, the specificity of these signs is still less than 90%, and on the other hand, most malignant lymph nodes do not exhibit all these signs simultaneously. EUS-FNA represents the current gold standard and has replaced more invasive procedures such as mediastinoscopy, at least for those groups of lymph nodes that are in reach of the EUS. In case of trained investigators, EUS-FNA reaches a sensitivity, specificity, and diagnostic accuracy of more than 90%. Hocke and colleagues had investigated a total of 122 patients with enlarged mediastinal and/or paraaortic lymph nodes diagnosed by CT. EUS-FNA was performed, and cytologic specimens were diagnosed as representing a malignant or benign process in case of Papanicolaou IV and V or Papanicolaou I and II, respectively. Based on cytologic results, the investigated lymph nodes were classified as neoplastic (n = 48) or nonneoplastic. Using the B-mode criteria, the preliminary diagnosis was confirmed in 64 of 74 benign lymph nodes (specificity 86%). Regarding malignant lymph nodes, 33 of 48 were confirmed (sensitivity 68%). Using the advanced CE-EUS criteria, the diagnosis was confirmed in 68 of 74 benign lymph nodes (specificity 91%). However, in case of malignant lymph nodes, the number of correct diagnoses reduced to 29 of 48 lymph nodes (sensitivity 60%). The CE-EUS criteria to identify benign lymph nodes and node enlargement in malignant lymphoma do not differ. If those 10 patients with malignant lymphoma are excluded, the sensitivity of the CE-EUS for malignant lymph nodes increases to 73%. CE-EUS improves the specificity in diagnosing benign lymph nodes as compared with B-mode EUS. It does not improve the correct identification of malignant lymph nodes and cannot replace EUS-FNA.
Summary
CE-EUS could provide a contribution to the differential diagnosis of a primary pancreatic carcinoma, chronic pancreatitis, and a pancreatic metastasis; therefore, CE-EUS can have a decisive influence on the selection of appropriate therapeutic strategies (eg, follow-up, chemotherapy, or surgery). However, histology remains the standard method in the differential diagnosis of pancreatic tumors. Regarding lymph nodes, CE-EUS cannot replace EUS-FNA.
Related posts:
 Endomicroscopy of Intestinal Metaplasia and Gastric Cancer
Endomicroscopy of Intestinal Metaplasia and Gastric Cancer
 Wide View and Retroview During Colonoscopy
Wide View and Retroview During Colonoscopy
 High-Definition Endoscopy and Magnifying Endoscopy Combined with Narrow Band Imaging in Gastric Cancer
High-Definition Endoscopy and Magnifying Endoscopy Combined with Narrow Band Imaging in Gastric Cancer
 New Options of Cholangioscopy
New Options of Cholangioscopy
 High-Definition and Filter-Aided Colonoscopy
High-Definition and Filter-Aided Colonoscopy
 Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors
Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


