Congenital Abnormalities
Cecal Agenesis
Intestinal agenesis is the failure of a portion of the enteric tube to form. This disorder is rare, occurring in 1 in 50,000 pregnancies. Males are more commonly affected than females. It can affect the rectosigmoid (where it associates with other major caudal anomalies) or the cecum. Cecal agenesis may result from misexpression of the endoderm-specific homeodomain gene IDX-1 (20). IDX-1 binds to CDX-2, the caudal homeodomain factor important in intestinal differentiation (21).
Malrotations
Most large intestinal malpositions (Fig. 13.20) accompany small intestinal malrotations that occur when the contents of the physiologic abdominal hernia return to the abdominal cavity (see Chapter 6). In malrotations, the cecum usually fails to rotate and lies in the left iliac fossa, in the midline of the pelvis, or in the upper abdomen. The ascending colon retains its mesentery and runs upward, just to the left of the midline, to lie below the gastric curvature, where a loop of transverse colon connects to a normally situated descending colon. When rotation occurs beyond 180 degrees, the colon crowds into the left side of the abdomen or the cecum assumes an unfixed position in the right upper quadrant. The transverse colon and splenic flexure may lie posterior to the stomach and anterior to all or part of the pancreas, a location known as pancreatic interposition. They may also lie in a retrosplenic location (22). The entire malpositioned bowel remains unanchored, supported by a single mesentery with a very narrow base that predisposes it to undergo intestinal volvulus (22). The body attempts to correct the unstable state of the malpositioned intestine by forming fibrous bands or adhesions between abdominal
structures. These bands and adhesions become sources of future problems.
structures. These bands and adhesions become sources of future problems.
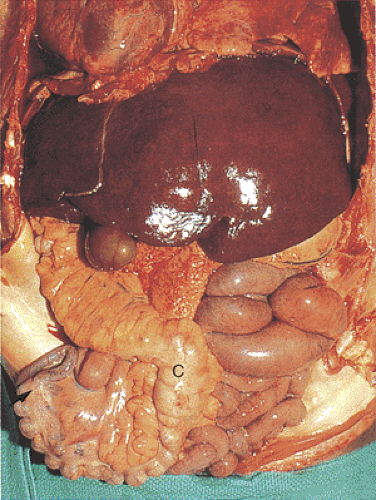 FIG. 13.20. Colonic malrotation. The colon (C) lies to the right of the midline and the small bowel lies to the left. |
Atresia and Stenosis
Large intestinal atresias and stenoses (Fig. 13.21) occur far less commonly than esophageal, small intestinal, or anal atresias. Atresias of the ascending and transverse colon develop more commonly than distal ones. Colonic atresia may coexist with other gastrointestinal or laryngeal atresias, gastroschisis (23), and Hirschsprung disease (24).
Hereditary multiple gastrointestinal atresias affect the gut from the pylorus to the rectum. Patients with multiple intestinal atresias may also have biliary atresia (23) or immunodeficiency syndromes (25). Cardiovascular and other gastrointestinal malformations constitute the most common associated major abnormalities; these are a major cause of morbidity and mortality. Skeletal and limb defects account for the most common minor anomalies. Atresias and stenoses are described in detail in Chapter 6.
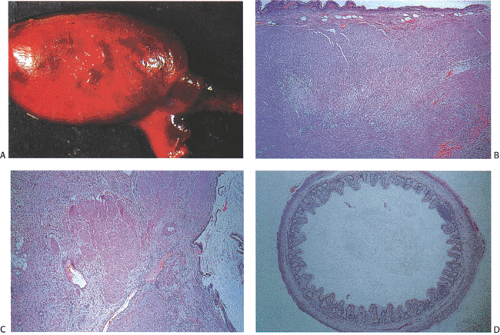 FIG. 13.21. Colonic atresia. A: The atresia is immediately adjacent to a colonic duplication. The bowel proximal to the duplication is massively dilated. B: Histologic section through an area of duplication showing the architectural abnormalities of the wall. C: At the right a small portion of the lumen is identified. It contains a vastly simplified colonic mucosa. D: Section through one of the duplicated segments of the bowel. The crypts are simplified, although the basic structure is preserved. Lymphoid follicles are present. The muscular coats are incomplete. |
Duplications, Congenital Diverticula, and Enterogenous Cysts
Large intestinal duplications (Fig. 13.22), congenital diverticula, and enterogenous cysts are related defects (Fig. 13.23) that affect both children and adults. They resemble their small intestinal counterparts described in Chapter 6. There is partial or complete formation of a second luminal structure with its own mucosa and submucosa and incomplete separation of the muscular walls of the two tubes. The duplication always lies on the antimesenteric aspect of the bowel.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


