CHAPTER 27 Complications of adjustable gastric banding
Step 1. Surgical anatomy
♦ Band complications can occur early or late. The most common late complications are port or tubing problems (2% to 3%), band slippage (3% to 6%), and band erosion (0.5% to 1%). We will concentrate on band slippage and band erosion in this chapter.
♦ In revisional operations, caution should be paid to the left gastric artery, or an aberrant left hepatic artery arising from the left gastric. These relatively large vessels can be obscured by a dense inflammatory reaction and may be unrecognized when dissecting to the left of the stomach and band buckle.
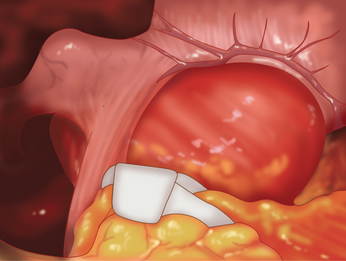
♦ The operative treatment of band slippage involves laparoscopic reduction of the herniated stomach, with band replacement or repositioning. This is usually possible via a laparoscopic approach. Contrast swallow shows an eccentric pouch enlargement above the band and that the angle of the band to the vertical is greater than 90 degrees (Figure 27-1 and 27-2).
♦ A hiatal hernia is commonly found in association with a band slip and should be repaired at the time of revisional surgery. Exploration reveals a dilated, eccentric gastric pouch above the band (Figure 27-2).

Step 2. Preoperative considerations
Patient preparation
♦ The modern technique of band placement is the pars flaccida approach, favored because of a decreased incidence of posterior band slippage. There is minimal posterior dissection at the level of the confluence of the left and right diaphragmatic crura. The posterior position of the band is at or just below the esophagogastric junction. Anteriorly a small (15 mL) virtual pouch is created.
♦ All patients should have a reassessment of their comorbidities and nutritional state before undergoing revisional bariatric surgery. Patients may develop anemia after band slippage secondary to erosive gastritis in the dilated pouch.
♦ Diagnosis and anatomy should be well defined preoperatively; the investigation of choice for band slip is a contrast swallow, and for band erosion it is an upper endoscopy.
Step 3. Operative steps
Access and port placement





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


