Color Plates
Plate 1.
Rectal mucosal biopsy specimen from a patient with dysentery caused by shigellosis. There is considerable mucosal inflammation caused by infiltration with polymorphonuclear leukocytes and mononuclear cells, as well as substantial damage to surface epithelial cells. However, mucosal architecture is generally preserved with straight, closely adjacent crypts. A crypt microabscess is seen on the right.
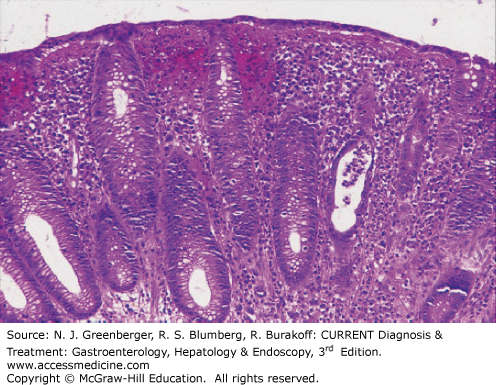
Plate 2.
Rectal mucosal biopsy specimen from a patient with dysenteric stools caused by a flare of chronic ulcerative colitis. The mucosa is heavily infiltrated with polymorphonuclear leukocytes and mononuclear cells. In contrast to Plate 1, mucosal architecture is markedly distorted, with substantial reduction in crypts and distortion of those that remain.
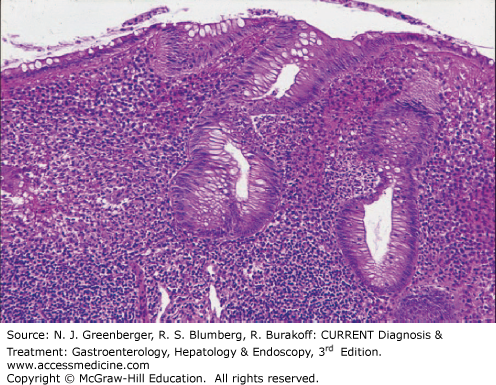
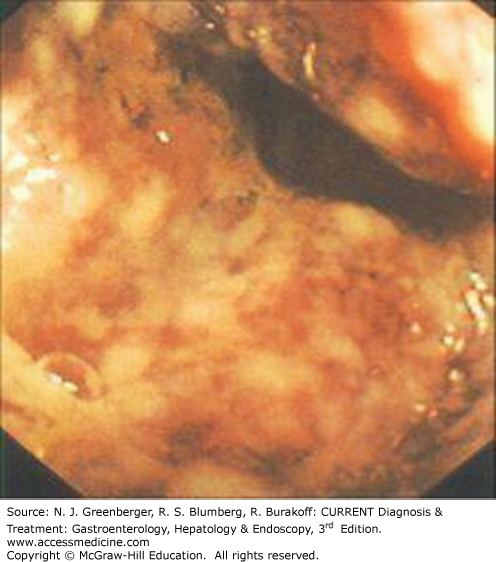
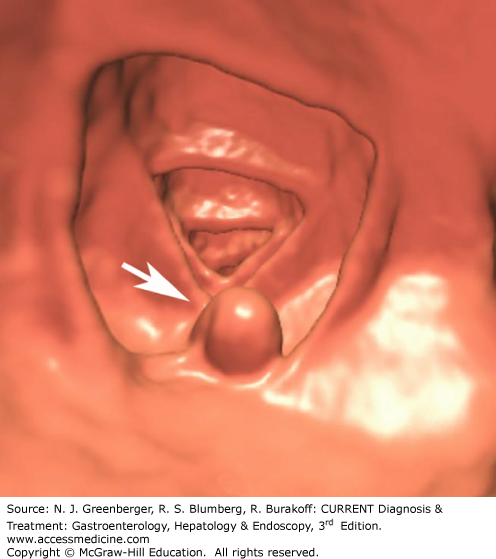
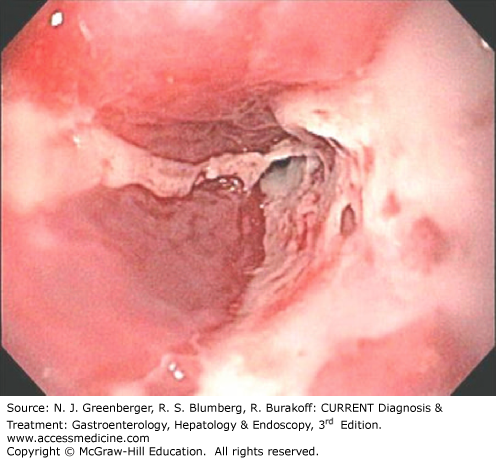
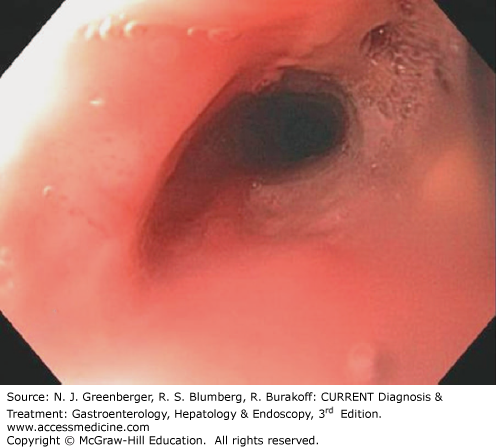
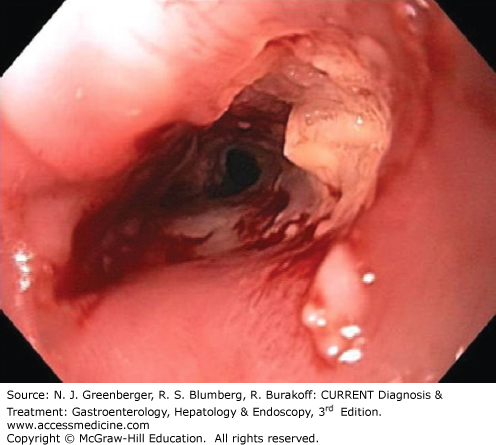
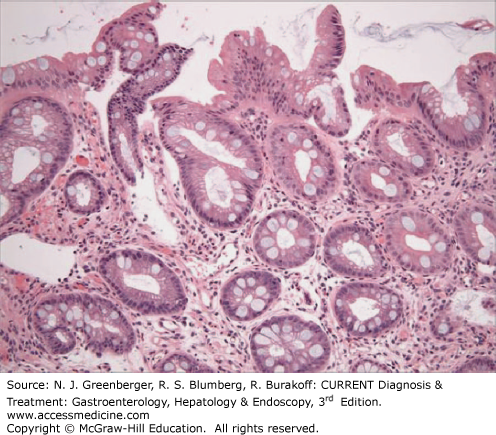
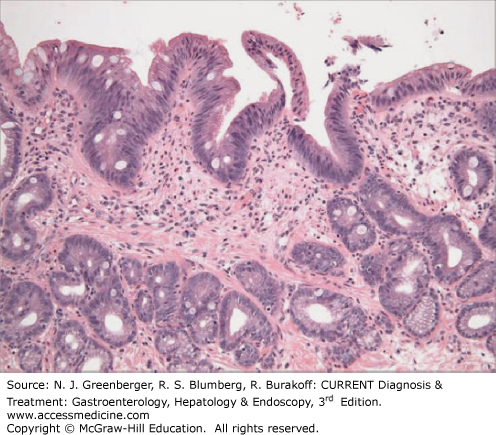
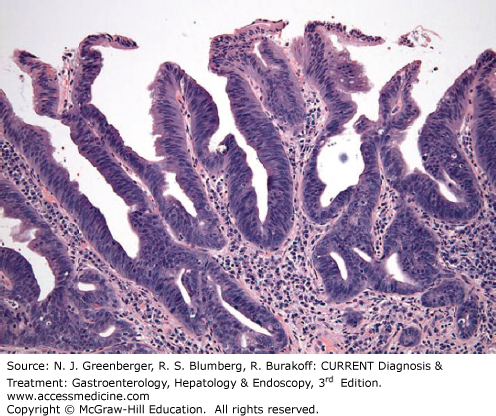
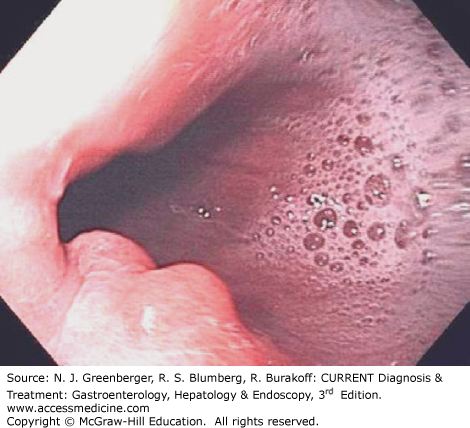
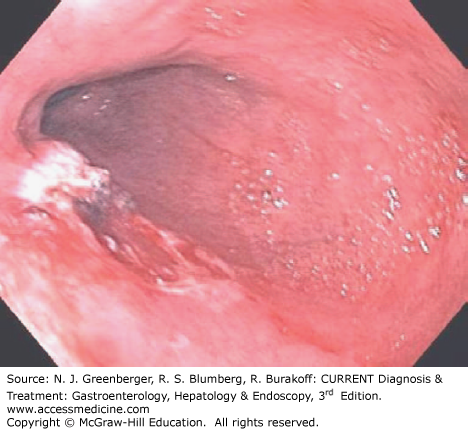
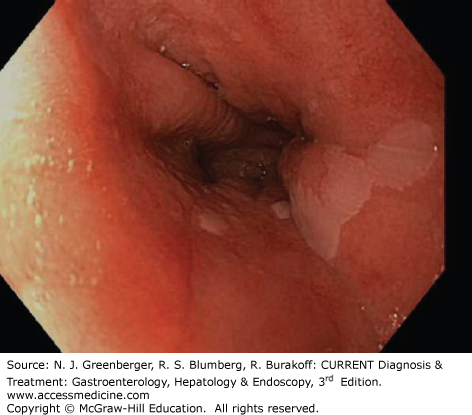
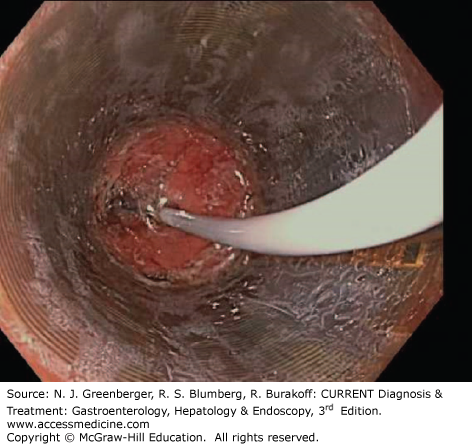
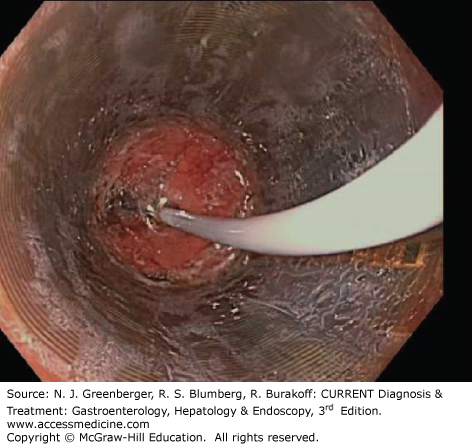
Plate 21.
The upper panel shows a characteristic severe lesion from a patient with untreated celiac sprue. Villi are absent, crypts are hyperplastic, and the lamina propria is infiltrated with many mononuclear cells. For comparison, the lower panel shows a biopsy sample from a normal volunteer showing normal mucosal architecture with tall villi and shallow crypts and just a few mononuclear cells in the lamina propria.
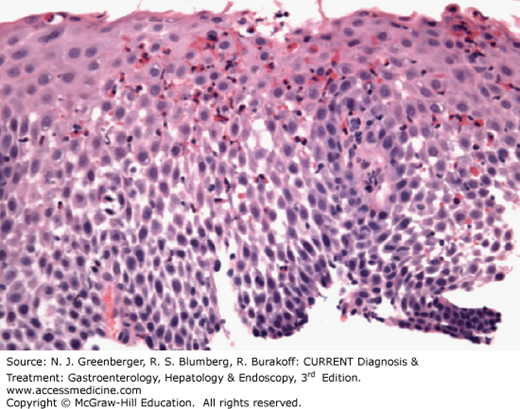
Plate 22.
The left panel shows at higher magnification the absorptive surface of the biopsy sample from the patient with celiac sprue shown in the upper panel of Plate 21. The surface absorptive cells are decreased in height and vacuolated, and the nuclei have lost their polarity. Numerous intraepithelial lymphocytes (IELs) can be seen between adjacent epithelial cells. The underlying lamina propria is heavily infiltrated with lymphocytes and plasma cells. For comparison, in the panel on the right is the tip of a villus from the biopsy sample shown in lower panel of Plate 23 from a normal individual. In contrast to the panel on the left, the absorptive cells are tall and have a well-developed brush border, with only occasional IELs evident between epithelial cells.
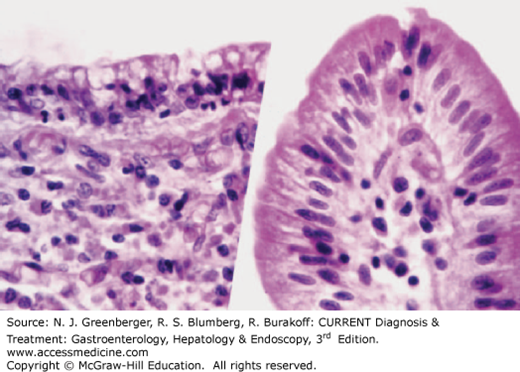
Plate 23.
Upper panel shows a biopsy sample obtained from a normal volunteer and stained with periodic acid–Schiff (PAS) stain. The glycoprotein-rich epithelial cell brush border and the goblet cell mucous are PAS-positive. The biopsy sample in the lower panel was obtained from a patient with untreated Whipple disease. The villus architecture is markedly distorted and the lamina propria is packed with large PAS-positive macrophages that virtually replace the lymphocytes and plasma cells that would normally be seen. Additionally, profiles of dilated lymphatics are evident in the lamina propria.
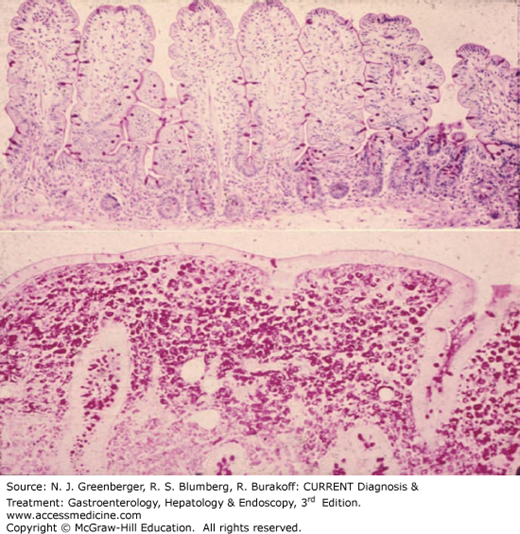
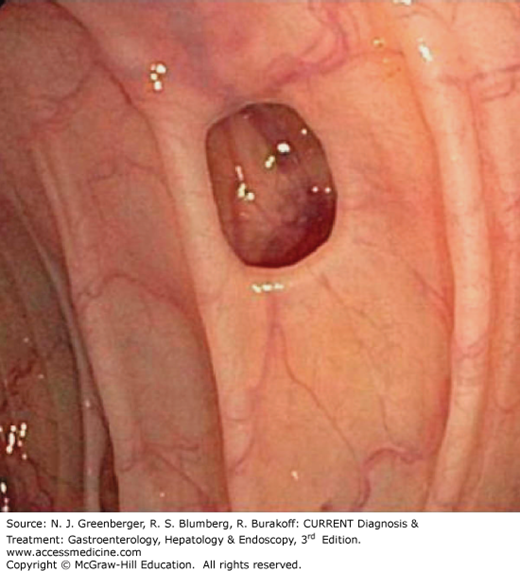
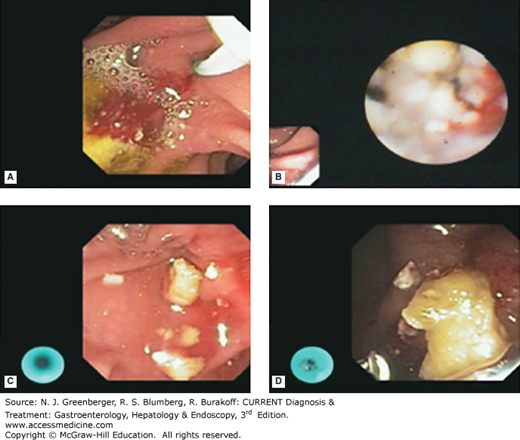
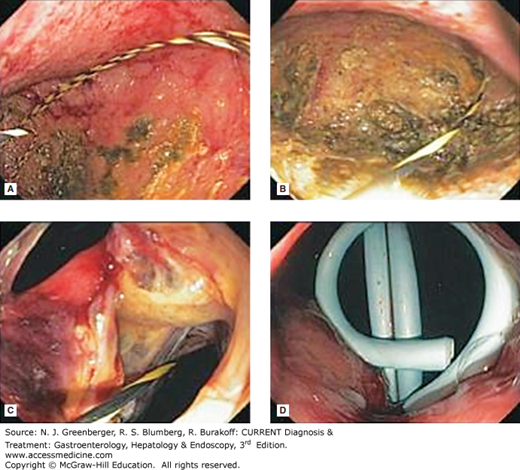
Plate 27.
Stepwise images (Plates 26, A–D and 27, A–D) of endoscopic drainage of symptomatic pancreas. A. pseudocyst, B. wire in cyst cavity, C. cystogastrostomy site with wire, D. residual pigtail catheters. (Used with permission from Christopher Thompson, MD.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


