Colonoscopic polypectomy is fundamental to effective colonoscopy. Through its impact on the polyp-cancer sequence, colonoscopic polypectomy reduces colorectal cancer incidence and mortality. Because it eliminates electrosurgical risk, cold snaring has emerged as the preferred technique for most small and all diminutive polyps. Few clinical trial data are available on the effectiveness and safety of specific techniques. Polypectomy technique seems highly variable between endoscopists, with some techniques more effective than others are. Further research is needed to investigate operator variation in polypectomy outcomes and establish an evidence base for best practice.
Key points
- •
Colonoscopic polypectomy is fundamental to effective colonoscopy.
- •
Operator variability influences the quality of colonoscopy for both detection and resection.
- •
Multiple questions remain about best practice techniques for colonoscopic polypectomy. Cold snaring seems to offer safe, effective, and efficient resection for small and diminutive polyps.
- •
Further research is urgently needed to investigate the apparent variation in polypectomy outcomes, and establish an evidence base for effective polypectomy.
Introduction
Polypectomy is fundamental to the practice of colonoscopy. The importance of polypectomy derives from the natural history of colorectal cancer (CRC) and its disruptive impact on the polyp-cancer sequence. By removing cancer precursors, polypectomy reduces CRC incidence and mortality. Data on the therapeutic benefit of colonoscopic polypectomy are derived from indirect evidence and longitudinal observational studies. Indirect evidence includes a population-level reduction in overall CRC incidence, likely due to CRC screening. Longitudinal evidence includes the adenoma-cohort studies in which long-term follow-up after adenoma removal in the National Polyp Study and other international cohort studies demonstrated a reduction in CRC incidence and mortality.
Introduction
Polypectomy is fundamental to the practice of colonoscopy. The importance of polypectomy derives from the natural history of colorectal cancer (CRC) and its disruptive impact on the polyp-cancer sequence. By removing cancer precursors, polypectomy reduces CRC incidence and mortality. Data on the therapeutic benefit of colonoscopic polypectomy are derived from indirect evidence and longitudinal observational studies. Indirect evidence includes a population-level reduction in overall CRC incidence, likely due to CRC screening. Longitudinal evidence includes the adenoma-cohort studies in which long-term follow-up after adenoma removal in the National Polyp Study and other international cohort studies demonstrated a reduction in CRC incidence and mortality.
Variation in colonoscopy and polypectomy effectiveness
Despite this potential, colonoscopy is not perfect. It is now clear that colonoscopy does not offer complete protection against CRC, particularly in the proximal colon. Interval (postcolonoscopy) cancers are clearly associated with the quality of colonoscopy performance. The factors contributing to this variation in effectiveness are multiple, including inadequate bowel preparation, incomplete insertion, and tumor biology, including the serrated pathway of neoplasia.
However, individual operator factors are likely the most important contributor. Studies show wide variation in levels of adenoma detection and serrated polyp detection between endoscopists and a clear relationship between adenoma detection and rates of interval cancer. Also, interval cancers are more commonly due to missed, than new lesions.
Emerging data extend this issue of operator variation to the effectiveness of polypectomy. It has been estimated that up to 27% of interval cancers may be due to incomplete endoscopic resection. The recent Complete Adenoma Resection (CARE) study has cast substantial doubt on the effectiveness of routine polypectomy techniques for complete histologic eradication. It showed high rates (over 10%) of incomplete hot snare resection of nonpedunculated neoplastic polyps (5–20 mm) and, importantly, rates of incomplete resection that varied significantly between endoscopists (6.5%–22.7%). Serrated polyps were a particular problem because they were almost four times more likely to be incompletely resected than adenomas (relative risk 3.74, 95% CI 2.04–6.84), with an incomplete resection rate approaching 50% for large serrated lesions. Other studies have questioned the effectiveness of resection with a biopsy forceps, with incomplete adenoma resection rates of up to 38%.
General principles of polypectomy
This variation in polypectomy outcomes indicates that some techniques are more effective than others are. It also highlights the relative lack of research attention and training on polypectomy techniques. As a result, recommendations regarding polypectomy technique are limited by a lack of evidence and are based on expert opinion and uncontrolled observational studies. Few clinical trial data have been available on the effectiveness and safety of specific techniques, and most have focused on postpolypectomy bleeding. Only recently have animal and clinical trials begun to define an evidence-base for basic polypectomy technique.
Most endoscopists, therefore, perform polypectomy as they were taught in fellowship or from expert commentary at postgraduate training courses. A 2004 survey of US gastroenterologists demonstrated substantial variation in polypectomy practices for lesions less than 10 mm. For example, for resection of polyps 4 to 6 mm, hot snare was used by 59%, cold snare by 15%, cold biopsy forceps by 19%, and hot biopsy forceps (HBF) by 21%.
The goals of colonoscopic polypectomy are the effective, safe, and efficient resection and retrieval of precancerous lesions. Techniques to accomplish these goals must completely eradicate pathologic tissue while minimizing the risk of complications, specifically perforation and hemorrhage. Most complications from colonoscopy (with experienced operators) are related to polypectomy. Further, because of the prevalence of small polyps, most polypectomy complications result from their removal. Polypectomy complications are also more likely with an increasing number and size of resected polyps and proximal location.
Polypectomy is difficult to learn, requiring skills in instrument handling including the ability to precisely and efficiently control the instrument tip and therapeutic devices. It is an important element of the overall task of colonoscopy, yet colonoscopy competency assessment has tended to focus on insertion skills and measurement of completion or intubation rates. It is likely that polypectomy skills require a baseline level of competence at instrument handling and tip control, although this has not been clarified. Specific polypectomy competencies have been defined only recently.
Within the limits of the current evidence base and lack of formal recommendations, this article describes current techniques and discusses controversies for basic colonoscopic polypectomy.
Techniques for resection of small and diminutive polyps
Small polyps are very common. Most (>90%) colorectal polyps are less than 10 mm. High-level adenoma detectors are now able to consistently achieve adenoma prevalence rates of approximately 40% to 50% in patients who have index screening colonoscopies. Therefore, effective techniques to remove these lesions must be optimized.
Cold forceps are readily applied to diminutive polyps, 3 mm or less, and are virtually without risk. However, cold forceps removal is associated with high rates of incomplete resection, particularly with increasing polyp size when multiple bites are more likely required. Piecemeal forceps resection limits visualization of any remaining adenomatous tissue due to blood contamination of the biopsy defect, which makes complete resection much less likely. The use of large capacity forceps that allow the polyp to be completed engulfed by the forceps and removed in a single piece may mitigate this risk. However, it seems that even jumbo forceps are associated with high rates (18%) of residual adenoma on postresection biopsy sampling.
The addition of electrocautery to forceps removal is intended to ensure tissue destruction. However, in practice, this benefit is not realized. In particular, HBF are not effective, with high rates of incomplete resection (up to 30%), even for polyps less than 5 mm. Also, HBF are associated with unacceptable rates of complications, notably uncontrolled, asymmetric, and transmural thermal injury to the colonic wall, resulting in perforation and rates of delayed postpolypectomy hemorrhage. HBF should certainly not be used for polyps greater than 5 mm because of the risk of residual adenoma and, in the author’s view, cannot be recommended at all.
I never use HBF, I use cold forceps sparingly, and I aim to avoid piecemeal cold forceps resection. It is my practice to use large-capacity cold forceps for only the most tiny, diminutive of polyps (1–2 mm) that can be removed in a single bite, often by only partly opening the forceps to facilitate polyp entrapment. They seem most useful when the polyp is relatively inaccessible for efficient snaring; for example, located in the left field of endoscopic view and/or cannot be easily repositioned for snare placement (because of instrument looping or specific location at a flexure).
Cold snaring is the preferred technique for virtually all small (<10 mm) and most diminutive (≤5 mm) polyps. It is now well established as a safe and efficient technique for lesions less than 10 mm. Cold snaring allows efficient resection of polyp tissue in a single piece, with a margin of normal tissue to ensure complete eradication. It is readily applied to most polyps less than 10 mm. Occasionally, polyps less than 10 mm are narrow-based and bulky or pedunculated. In these occasional situations, hot snare resection may be warranted because of the higher risk of immediate bleeding with a more vascular pedicle.
Like cold forceps, cold snaring is essentially without risk. Bleeding is typically minor, immediate, and insignificant. The advantage of cold techniques is the capacity to visualize immediately any significant bleeding from injury to submucosal vessels (which is the usual cause of delayed bleeding). As a result, cold snaring can be regarded as safe in patients taking antiplatelet agents or therapeutic anticoagulation. A large Italian observational study of 1015 consecutive polyps confirmed the safety of cold techniques for polyps less than 10 mm, showing a low rate of immediate bleeding (1.8%), and no delayed bleeding or perforation. Antiplatelet agents (aspirin, ticlopidine) predicted bleeding, although patients taking clopidogrel were excluded. Other small studies suggest that cold snaring may be more efficient than hot snaring.
The effectiveness of cold snaring for polyp resection has not been well studied. Observational data suggest it may be more effective than forceps techniques, yet its effectiveness compared with hot snaring has not been evaluated in prospective randomized studies. The recent CARE study casts doubt on the effectiveness of hot snare polypectomy, which is unresolved for cold snaring. Studies comparing the completeness of polyp resection for cold versus hot snaring are required.
Cold Snaring
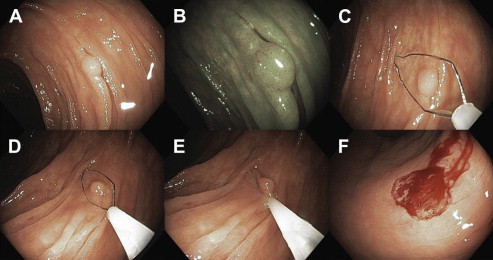
The technique of cold snaring is fundamentally different from snaring with electrocautery ( Fig. 1 , Table 1 , [CR] ). With hot snaring, capturing excess tissue around the polyp should be avoided and, once snared, the lesion should be lifted into the lumen by tenting the sheath away from the colon wall, to avoid electrocautery injury to the colon wall. With cold snaring, the goal is to capture and resect a 1 to 2 mm margin of normal tissue around the polyp. To achieve this, and to prevent the polyp specimen from flying away, the snare sheath should remain embedded within the colon wall during snare closure. The endoscopist should advance the sheath to at least 2 mm of the distal edge of the polyp and keep the sheath in this position while the snare is full closed around the polyp and the tissue guillotined. This may require gentle forward pressure on the snare sheath (or instrument) or angulation of the instrument tip into the wall (typically downward and right tip angulation) during snare closure. Suction can help the snare to capture the polyp and surrounding tissue. Next, the snare is gradually and completely closed in a single, continuous movement to guillotine the tissue. Once the tissue has been transected, the polyp tissue typically remains within or adjacent to the polypectomy defect, if the sheath has not been lifted during snare closure. The polyp can then be readily suctioned and retrieved.
| Cold Snaring | Hot Snaring | |
|---|---|---|
| Margin of normal tissue | Yes: at least 1–2 mm | Minimal |
| Tenting of lesion | No: snare sheath should remain pressed against colon wall | Yes: for application of electrocautery |
| Snare closure | Continuous until polyp guillotined | Snare closure stopped once resistance detected (or mark on snare handle reached) |
| Air aspiration | Not essential (can help snare to grasp polyp) | Yes |
| Electrocautery | No | Yes |
Precise and efficient manipulation of the snare sheath and wire requires skill in tip control. For additional control of the instrument tip, particularly for simultaneous movement of the snare, angulation controls, and insertion tube (forward or back), consider stabilizing the insertion tube between the fourth and fifth fingers of the left hand (the left-hand scope grip). This frees the right hand to manipulate the snare sheath within the instrument channel, or the right or left angulation control for additional tip control.
Snare choice has an impact on the ease and efficiency of cold snaring, although evidence is lacking. Most experts use diminutive minisnares (9–15 mm), including snare shapes that facilitate capturing a rim of normal tissue around the lesion. The diameter (thickness) of the wire is also relevant because it affects the ease of cold transection. For snare closure, some endoscopists advocate marking the snare handle to assist in estimating the amount of tissue ensnared. This is typically not required with cold snaring because there is no requirement to pause once the snare is closed around the polyp. Rather, after the polyp is encircled, the snare is gradually and completely closed and the polyp is guillotined in a single, continuous, and controlled movement of the snare handle. This is distinct from hot snaring in which inadvertent guillotining of the polyp before the application of electrocautery must be avoided.
Occasionally, the snare may fail to cut through and guillotine the tissue. If this occurs, it is likely that the snare has captured some submucosa, which is preventing complete transection ( Fig. 2 ). Failure to cold transect may occur more often with broader based polyps (approaching 10 mm), although can occur when excess normal tissue has been captured adjacent to a small polyp. In my experience, it does seem to happen less often with thin wire mini snares or dedicated cold snares. At this point, it is best to avoid application of electrocautery because of the risk of thermal injury to submucosal vessels and delayed bleeding. My approach is to keep the snare tightly closed and wait a few seconds because the snare will often slowly transect the tissue. If not, with the snare tightly closed, cautiously lift the snare away from the colon wall, attempting to encourage release of the entrapped submucosa. Sometimes, this may require slight relaxation of the snare wire, although it is best to avoid fully reopening the snare because the margin of normal mucosa may be lost or the polyp may be resected piecemeal.

Cold snaring allows rapid and immediate visualization of the polypectomy defect after resection. The margins of the defect can be quickly inspected to confirm complete resection. There is typically minor capillary bleeding after cold resection, which is trivial and not clinically significant. Very occasionally, there is more prominent bleeding streaming from the base of the defect, usually in patients with coagulopathy or therapeutic anticoagulation. The benefit of cold snaring is the immediate visualization of any significant bleeding, which can be readily treated with clips.
Pedunculated Polyps
Pedunculated polyps require a different technique, more typical of traditional hot snare polypectomy. The snare should be carefully positioned around the stalk approximately one-half to one-third the distance between the polyp head and the colon wall, allowing sufficient resection margin in case of malignancy within the polyp head and leaving sufficient stalk tissue to regrasp in the event of bleeding. Access to the lesion should be optimized, and it is advisable to consider repositioning the patient so that the stalk attachment is not in a dependent segment of the colon. This allows ready visualization and access to the stalk in the event of immediate postresection bleeding. Once snared, the lesion should be lifted away from the colonic wall, being careful to minimize contact with the opposing colonic wall to avoid contralateral electrocautery injury. For large pedunculated lesions, ancillary strategies to prevent postpolypectomy bleeding should be considered (see the article by Sanchez-Yague and colleagues elsewhere in this issue).
Uncertainties and controversies
The Use of Electrocautery
Traditionally, electrosurgical current (electrocautery) has been used in combination with mechanical transection for resection of all polyps with either snare or biopsy techniques. Electrocautery simultaneously ensures acute hemostasis while providing thermal fulguration of the polypectomy margins to ensure obliteration of pathologic tissue. The snare prevents blood flow by mechanically coapting blood vessel walls while heat seals the vessels closed.
However, the optimal choice of electrosurgical current is unresolved. There are few data to guide decisions regarding current or other electrosurgical settings, and power outputs between electrosurgical generators are not easily compared. Many experts have advocated pure low-power coagulation, which provides good immediate hemostasis, but likely a higher chance of transmural thermal injury and a higher rate of delayed bleeding. Blended current achieves effective transection with a lower depth of thermal injury and delayed bleeding, although rates of immediate bleeding are higher. Improvements in technology have seen the introduction of more sophisticated electrosurgical generators in which power output is microprocessor-controlled and responsive to tissue impedance. Output power is adjusted automatically and applied cyclically, alternating between cutting and coagulation current to minimize depth and spread of thermal injury. Many endoscopists have begun to use these systems for complex polypectomy. The contribution of type of electrosurgical current to variable polypectomy effectiveness is unknown.
However, electrocautery is responsible for virtually all of the complications associated with polypectomy. The risk of complications increases with the number of polypectomies performed with electrocautery. As a result, cold mechanical techniques have become the preferred strategy for small and diminutive polyps.
Resection of Serrated Polyps
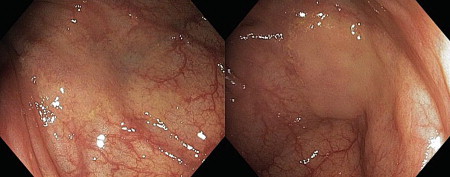
Serrated polyps (specifically, sessile serrated adenoma or polyp [SSA/P]) pose a particular problem for colonoscopy and polypectomy. They are likely significant contributors to postcolonoscopy interval CRC due to failures in detection, but also failures in resection as highlighted by the CARE study. SSA/P are typically flat subtle lesions draped over or thickening folds, with a yellow-brown mucus cap. They have characteristically indistinct margins that blend imperceptibly with normal mucosa ( Fig. 3 ), particularly when their mucus cap is removed.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


