Advancements in image technology have allowed recognition of mucosal architecture in more detail and may improve adenoma detection. This review provides a technical overview on individual imaging technologies and their effect on detection of adenomas. Only high-definition endoscopy has been shown to improve detection of small adenomas. None of the digital chromoendoscopy technologies improves adenoma detection. Limited studies on autoimmunfluorescence imaging in conjunction with high-definition endoscopy may improve detection of small adenomas.
Key points
- •
Advancements in image technology have allowed recognition of mucosal architecture in more detail and may improve adenoma detection.
- •
This review provides a technical overview on individual imaging technologies and their effect on detection of adenoma.
- •
High-definition white light endoscopy improves detection of small adenomas.
- •
None of the digital chromoendoscopy technologies improves adenoma detection.
- •
Autoimmunfluorescence imaging in conjunction with high-definition endoscopy may improve detection of small adenomas.
The effector of benefit for all colorectal cancer (CRC) screening modalities is colonoscopy with adequate detection and resection of neoplastic polyps. It is therefore neoplasia detection that determines screening efficacy. However, several studies have shown that many adenomas are missed during a colonoscopy, with an overall miss rate of approximately 20%, ranging from 6% for large (≥10 mm) adenomas to 13% for small (6–9 mm) and 26% for diminutive (≤5 mm) adenomas. Missing neoplastic lesions likely represents the major contributor to the development of postcolonoscopy or so-called interval cancers in as many as 70% to 80% of patients. Minimizing miss rate and improving neoplasia detection may therefore be regarded as the most important task to improve the effectiveness of CRC screening. This objective has been well recognized by gastrointestinal societies, and adenoma detection rate is considered a key quality indicator of colonoscopy.
Considerable advancements in endoscopic imaging technology may improve detection. In 1869, when Adolf Kussmaul performed the first documented upper endoscopy on a sword swallower, he did not have adequate light to recognize intestinal epithelium. Through integrated lenses and mirrors (Schindler-Wolf gastroscope 1932), fiber-optic bundles (Hirshowitz 1957), and camera chips with transmission of digital images, we have entered a new phase in endoscopic imaging. We have now at our disposal high-resolution endoscopes with various imaging filters, capable of postimage processing with the common goal of better recognizing intestinal disease.
In this article, the following advanced imaging technologies are discussed:
- •
High-definition (HD) colonoscopy
- •
Narrow-band imaging (NBI) (Olympus Medical Systems, Tokyo, Japan)
- •
Fujinon Intelligence Chromoendoscopy (FICE) (Fujinon Inc, Saitama, Japan)
- •
i-Scan (Pentax, Tokyo, Japan)
- •
Autofluorescence imaging (AFI) (Olympus Medical Systems, Tokyo, Japan)
The goal is to provide a technological update and to summarize whether and to what extent these imaging modalities improve detection of neoplastic polyps. Each section reviews the technology, summarizes studies on adenoma detection, and provides an outlook for next steps and potential areas for research.
High-Definition endoscopy
When camera chips replaced fiber-optic bundles, the operator was able to view video-transmitted images in real time on a monitor. Camera chips are charged coupled devices (CCD) comprising several thousands of photo cells known as picture elements (pixels). Pixel density has substantially increased in recent years. Whereas first-generation video endoscopes were equipped with 200,000-pixel CCDs, current endoscopes contain chips with 1.4 million pixels, allowing high image resolution.
Current Olympus endoscopes use 1 of 2 imaging systems. In the LUCERA system (Olympus 200 series, used in Asia and the United Kingdom) light from a xenon arc lamp is filtered through a rotating broadband red-green-blue filter to produce sequential light bursts in each spectrum. The reflected red, blue, and green images are sequentially captured by a monochromatic CCD and transmitted to a video processor to create a single composite picture in full color ( Fig. 1 A).
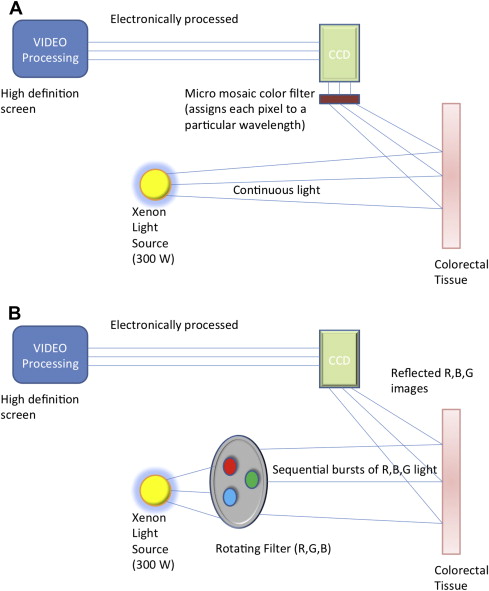
In contrast, the EXERA system (Olympus 100 series, used in North and South America and in many European countries) uses full-spectrum white light (WL) from a xenon lamp. The light is reflected off the mucosa and passes through a color filter mounted over the CCD. The filter selectively assigns each wavelength to a particular pixel, hence creating an image on the CCD surface. The image is then processed and displayed (see Fig. 1 B).
To enhance image acquisition and processing, high-resolution images can be shown on HD monitors. The standard broadcasting systems (PAL [phase alternating line] and NTSC [National Television Standard Committee]) generate approximately 48 to 576 scanning lines on a screen, whereas the new HD monitors generate up to 1080 scanning lines. These HD endoscopy systems (high-resolution endoscopy combined with HD screens) therefore allow examination of the mucosal architecture in the gastrointestinal tract.
Summary of Studies on High-Definition Colonoscopy and Adenoma Detection
Because HD colonoscopy shows mucosal surface in greater detail, it is plausible that it may improve neoplasia detection. Of 8 published studies ( Table 1 ) 3 were randomized controlled trials (RCTs) and 2 did not shown a significant benefit ; however, both RCTs seem to have been underpowered. For instance a clinically meaningful improvement in adenoma detection rate (ADR) from 50% to 58% with HD in the study by Tribonias and colleagues was not statistically significant. A third randomized trial by Rastogi and colleagues found an improved ADR from 39% to 46%, but again this was not significant ( P = .17). This study found a significant increase of flat adenomas (9% vs 2%, P = .01) and right-sided adenomas (34% vs 19%, P = .01), but there was no benefit of HD for detection of advanced adenomas.
| Study | Method | Endoscopist (Center) | Patients | Population | ADR (%) | Mean Number of Adenomas per Patient | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| HD | HD | SD | P | HD | SD | P | ||||
| Pellise et al, 2008 | RCT | 7 (1) | 620 | Average | 26 | 25 | .96 | 0.45 | 0.43 | .87 |
| Tribonias et al, 2010 | RCT | 1 (1) | 300 | Average | 58 | 50 | .16 | 1.4 | 1.1 | .10 |
| Rastogi et al, , a 2011 | RCT | 6 (2) | 420 | Average | 46 | 39 | .17 | 1.13 | 0.69 | .02 |
| East et al, 2008 | Prospective nonrandomized | 1 (1) | 130 | Average | 71 | 60 | .20 | 1.6 | 1.2 | n.s. |
| Adler et al, 2012 | Prospective nonrandomized | 27 (23) | 1656 | Average | 22 | 18 | <.01 | 0.33 | 0.27 | <.01 |
| Buchner et al, 2010 | Retrospective | 18 (1) | 2430 | Average | 29 | 24 | .02 | 0.51 | 0.44 | .01 |
| Burke et al, 2010 | Retrospective | Multiple (1) | 852 | Average | 25 | 22 | .36 | 0.4 | 0.3 | .13 |
| Erim et al, 2011 | Retrospective (HD Fujinon vs SD Pentax) | 3 (1) | 900 | Average | 19 | 18 | .56 | 0.41 | 0.42 | .82 |
a 3 arms: HD, NBI, and SD (see Table 2 ).
The remaining 5 studies had different designs. Two were prospective, and 3 retrospective. Only 1 study examined non-Olympus colonoscopes, and compared an HD Fujinon with a standard-definition (SD) Pentax colonoscope. This study did not find a difference in adenoma detection. Despite a nonrandomized design, all studies attempted to compare groups that were similar to each other. For instance, one of the retrospective studies by Burke and colleagues compared 852 patients who were assigned to different scopes by availability. In this study, HD colonoscopes did not improve adenoma detection. Another retrospective study by Buchner and colleagues analyzed more than 1400 patients who were assigned to rooms with or without HD scopes. In this study, HD colonoscopy increased overall ADR from 24% to 29% ( P = .02), but it did not improve detection of advanced adenomas. Similar results were reported by Adler and colleagues, in a large prospective study from Germany, which compared 1256 patients from 5 clinical practices equipped with HD colonoscopes with 1400 patients from 18 practices using older SD colonoscopes. HD increased ADR from 18% to 22% ( P <.01), with a marginally significant increase in detection of adenomas with high-grade dysplasia from 0.6% to 1.2% ( P = .06).
Although nonrandomized, the major strength of these studies is the large sample size and the participation of multiple endoscopists, which reflects how these new colonoscopes fare in clinical practice. A recent meta-analysis systematically summarized 5 of the discussed studies. HD colonoscopy improved ADR in pooled analysis by 3.5% (95% confidence interval [CI] 0.9–6.1), largely related to an increased detection of diminutive adenomas. When also considering studies that were not included in the meta-analysis, the gain in ADR with HD would be even greater (crude increase of 4.4%).
The HD colonoscopes also come with an increased visual angle from 140° with prior Olympus scopes to 170°with HD scopes. Although it seems plausible that the increased angle may enhance adenoma detection, 3 studies that have examined wide-angle colonoscopy did not find that it improved adenoma detection.
High-Definition Colonoscopy: Summary and Outlook
Studies on HD colonoscopy showed the following main results:
- 1.
HD endoscopy improves adenoma detection.
- 2.
The increased adenoma detection is related to an improved detection of small adenomas. It does not improve detection of large or advanced lesions.
It may be argued that the reported increase in ADR is marginal. However, the approximate 4% absolute increase translates to a relative increase of 16% (from 28% to 33%). When we consider an adenoma miss rate of 20%, an increased adenoma detection by 16% with HD colonoscopy seems relevant.
Most endoscopy units have moved to HD systems and the next generation of HD endoscopy has been introduced. Although it is important to continue to assess whether they improve adenoma detection, studies should also examine whether higher-resolution colonoscopes might help to better recognize sessile serrated adenomas/polyps.
High-Definition endoscopy
When camera chips replaced fiber-optic bundles, the operator was able to view video-transmitted images in real time on a monitor. Camera chips are charged coupled devices (CCD) comprising several thousands of photo cells known as picture elements (pixels). Pixel density has substantially increased in recent years. Whereas first-generation video endoscopes were equipped with 200,000-pixel CCDs, current endoscopes contain chips with 1.4 million pixels, allowing high image resolution.
Current Olympus endoscopes use 1 of 2 imaging systems. In the LUCERA system (Olympus 200 series, used in Asia and the United Kingdom) light from a xenon arc lamp is filtered through a rotating broadband red-green-blue filter to produce sequential light bursts in each spectrum. The reflected red, blue, and green images are sequentially captured by a monochromatic CCD and transmitted to a video processor to create a single composite picture in full color ( Fig. 1 A).
In contrast, the EXERA system (Olympus 100 series, used in North and South America and in many European countries) uses full-spectrum white light (WL) from a xenon lamp. The light is reflected off the mucosa and passes through a color filter mounted over the CCD. The filter selectively assigns each wavelength to a particular pixel, hence creating an image on the CCD surface. The image is then processed and displayed (see Fig. 1 B).
To enhance image acquisition and processing, high-resolution images can be shown on HD monitors. The standard broadcasting systems (PAL [phase alternating line] and NTSC [National Television Standard Committee]) generate approximately 48 to 576 scanning lines on a screen, whereas the new HD monitors generate up to 1080 scanning lines. These HD endoscopy systems (high-resolution endoscopy combined with HD screens) therefore allow examination of the mucosal architecture in the gastrointestinal tract.
Summary of Studies on High-Definition Colonoscopy and Adenoma Detection
Because HD colonoscopy shows mucosal surface in greater detail, it is plausible that it may improve neoplasia detection. Of 8 published studies ( Table 1 ) 3 were randomized controlled trials (RCTs) and 2 did not shown a significant benefit ; however, both RCTs seem to have been underpowered. For instance a clinically meaningful improvement in adenoma detection rate (ADR) from 50% to 58% with HD in the study by Tribonias and colleagues was not statistically significant. A third randomized trial by Rastogi and colleagues found an improved ADR from 39% to 46%, but again this was not significant ( P = .17). This study found a significant increase of flat adenomas (9% vs 2%, P = .01) and right-sided adenomas (34% vs 19%, P = .01), but there was no benefit of HD for detection of advanced adenomas.
| Study | Method | Endoscopist (Center) | Patients | Population | ADR (%) | Mean Number of Adenomas per Patient | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| HD | HD | SD | P | HD | SD | P | ||||
| Pellise et al, 2008 | RCT | 7 (1) | 620 | Average | 26 | 25 | .96 | 0.45 | 0.43 | .87 |
| Tribonias et al, 2010 | RCT | 1 (1) | 300 | Average | 58 | 50 | .16 | 1.4 | 1.1 | .10 |
| Rastogi et al, , a 2011 | RCT | 6 (2) | 420 | Average | 46 | 39 | .17 | 1.13 | 0.69 | .02 |
| East et al, 2008 | Prospective nonrandomized | 1 (1) | 130 | Average | 71 | 60 | .20 | 1.6 | 1.2 | n.s. |
| Adler et al, 2012 | Prospective nonrandomized | 27 (23) | 1656 | Average | 22 | 18 | <.01 | 0.33 | 0.27 | <.01 |
| Buchner et al, 2010 | Retrospective | 18 (1) | 2430 | Average | 29 | 24 | .02 | 0.51 | 0.44 | .01 |
| Burke et al, 2010 | Retrospective | Multiple (1) | 852 | Average | 25 | 22 | .36 | 0.4 | 0.3 | .13 |
| Erim et al, 2011 | Retrospective (HD Fujinon vs SD Pentax) | 3 (1) | 900 | Average | 19 | 18 | .56 | 0.41 | 0.42 | .82 |
a 3 arms: HD, NBI, and SD (see Table 2 ).
The remaining 5 studies had different designs. Two were prospective, and 3 retrospective. Only 1 study examined non-Olympus colonoscopes, and compared an HD Fujinon with a standard-definition (SD) Pentax colonoscope. This study did not find a difference in adenoma detection. Despite a nonrandomized design, all studies attempted to compare groups that were similar to each other. For instance, one of the retrospective studies by Burke and colleagues compared 852 patients who were assigned to different scopes by availability. In this study, HD colonoscopes did not improve adenoma detection. Another retrospective study by Buchner and colleagues analyzed more than 1400 patients who were assigned to rooms with or without HD scopes. In this study, HD colonoscopy increased overall ADR from 24% to 29% ( P = .02), but it did not improve detection of advanced adenomas. Similar results were reported by Adler and colleagues, in a large prospective study from Germany, which compared 1256 patients from 5 clinical practices equipped with HD colonoscopes with 1400 patients from 18 practices using older SD colonoscopes. HD increased ADR from 18% to 22% ( P <.01), with a marginally significant increase in detection of adenomas with high-grade dysplasia from 0.6% to 1.2% ( P = .06).
Although nonrandomized, the major strength of these studies is the large sample size and the participation of multiple endoscopists, which reflects how these new colonoscopes fare in clinical practice. A recent meta-analysis systematically summarized 5 of the discussed studies. HD colonoscopy improved ADR in pooled analysis by 3.5% (95% confidence interval [CI] 0.9–6.1), largely related to an increased detection of diminutive adenomas. When also considering studies that were not included in the meta-analysis, the gain in ADR with HD would be even greater (crude increase of 4.4%).
The HD colonoscopes also come with an increased visual angle from 140° with prior Olympus scopes to 170°with HD scopes. Although it seems plausible that the increased angle may enhance adenoma detection, 3 studies that have examined wide-angle colonoscopy did not find that it improved adenoma detection.
High-Definition Colonoscopy: Summary and Outlook
Studies on HD colonoscopy showed the following main results:
- 1.
HD endoscopy improves adenoma detection.
- 2.
The increased adenoma detection is related to an improved detection of small adenomas. It does not improve detection of large or advanced lesions.
It may be argued that the reported increase in ADR is marginal. However, the approximate 4% absolute increase translates to a relative increase of 16% (from 28% to 33%). When we consider an adenoma miss rate of 20%, an increased adenoma detection by 16% with HD colonoscopy seems relevant.
Most endoscopy units have moved to HD systems and the next generation of HD endoscopy has been introduced. Although it is important to continue to assess whether they improve adenoma detection, studies should also examine whether higher-resolution colonoscopes might help to better recognize sessile serrated adenomas/polyps.
Digital chromoendoscopy
Light absorption and reflection are dependent on mucosal characteristics. Selecting certain wavelengths of reflected light or image processing may therefore contrast neoplastic from nonneoplastic tissue. Resultant images appear in a different color reminiscent of chromoendoscopy, therefore these electronically modified imaging modalities are also called electronic, virtual, or digital chromoendoscopy. Available systems differ in their technology, but result in a similar effect: enhancement of mucosal contrast. NBI filters light before image processing. In contrast, FICE and i-Scan manipulate light using postprocessing computer algorithms.
NBI
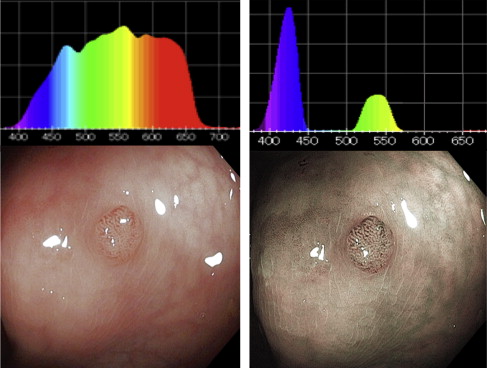
Conventional WL endoscopy uses the entire spectrum of visible light (400–700 nm) and allows viewing of mucosa in its natural color. NBI (Olympus) uses a light filter to achieve an increased proportion of blue light (that allows its passage) and a decreased proportion of red light (that does not allow its passage) ( Fig. 2 ). Therefore, it narrows standard WL to a bandwidth of blue light (390–445 nm) and green light (530–550 nm). This narrowed band spectrum corresponds to the main peaks on the absorption spectrum of hemoglobin; it is preferentially absorbed by hemoglobin and appears dark (not reflected), thus enhancing tissue microvasculature from its surrounding. In addition, the shorter wavelength of blue light has a more shallow tissue penetration than the longer wavelength of red light. Therefore, NBI enhances structures in the surface, especially those with hemoglobin content. Because adenomas have an increased vascular density and abnormal vascular pattern, NBI should help to improve detection of adenomatous polyps.
Studies on NBI and Adenoma Detection
At least 11 fully published randomized studies have examined whether NBI improves detection of adenoma or decreases the adenoma miss rate when compared with high definition white light (HDWL), either in average-risk screening and surveillance populations or in higher-risk individuals ( Table 2 ). The fact that at least 5 meta-analyses have been published on the subject highlights the interest in understanding whether NBI increases adenoma detection. The most recent is a Cochrane meta-analysis, which also includes 3 studies published only as an abstract. The overall results are clear: NBI does not improve adenoma detection and does not decrease the adenoma miss rate. In fact, none of the studies found a significant benefit of NBI compared with HDWL. One of the initial studies suggested that the use of NBI may assist in learning to better recognize adenomas with WL. The investigators observed an increasing ADR with WL during the study period. However, this was not supported by later studies. For instance, Rex and Helbig reported a very high ADR (66%) with either technology in a study by a single endoscopist. Such ADR in an average screening population was unprecedented and was higher than historical controls by the same endoscopist. The investigators speculate that it is not NBI alone, but rather HD imaging (with or without NBI) that improves adenoma detection. The benefit seems to be in finding more small and diminutive adenomas, which is also supported by studies comparing HD with SD colonoscopy (as discussed earlier). NBI did seem to improve the detection of flat adenomas in 2 studies, but showed a lower flat ADR in a third study. No effect was seen in the detection of small adenomas or advanced adenomas, or with respect to location in the colon. Some studies have noted a longer withdrawal time with NBI, yet no difference in adenoma detection, indicating that WL viewing was dominant over NBI (same number of adenomas in a shorter time).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


