Chapter 43 Choledocholithiasis
 Video related to this chapter’s topics:
Video related to this chapter’s topics:Introduction
Gallstone disease affects people of both genders from every society, race, and age group. It is estimated that 15% of Americans have gallstones. Approximately 700,000 cholecystectomies are performed each year in the United States, making it the most common reason for digestive disease admission to Western hospitals. More than 95% of biliary tract disorders are related to gallstones.1 Most bile duct stones are gallstones that have passed into the bile duct.
Cholelithiasis refers to gallbladder stones, and choledocholithiasis refers to stones in the bile ducts. Noncrumbling concretions larger than 2 mm in diameter are considered stones, and biliary microlithiasis refers to particles 2 mm or less in diameter, although there is no universally accepted definition. Choledocholithiasis can be classified as primary stones, which develop in the bile ducts, or secondary stones, which pass from the gallbladder. Choledocholithiasis can be subdivided further by the location of the stones, which may be intrahepatic or extrahepatic. Of patients with symptomatic gallstone disease, 5% to 15% have bile duct stones, yet greater than 90% of patients with choledocholithiasis also have cholelithiasis. Sludge is a suspension of cholesterol monohydrate crystals, calcium bilirubinate granules, and other calcium salts with or without microlithiasis in gallbladder mucus. Sludge is a form of gallstone disease and may predispose to macroscopic stones or cause pancreatitis and other morbidity directly.2
Cholelithiasis
Most gallstones are composed primarily of cholesterol and are nodular and round with a golden color. A few gallstones contain mostly calcium bilirubinate and are round, hard, and black. Primary bile duct stones are composed of calcium salts of unconjugated bilirubin with variable amounts of cholesterol, protein, and bacteria. These stones are brown, are amorphous, and have an earthy texture. Fig. 43.1 shows examples of stones extracted from the bile duct.

Choledocholithiasis
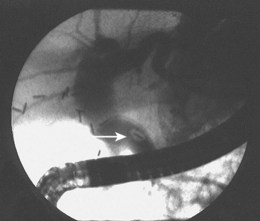
Epidemiologically, primary and secondary bile duct stones vary greatly. In Western societies, most bile duct stones are secondary, and the prevalence increases with age. Primary bile duct stones are more common in Asia. Primary stones are associated with bacterial contamination of the choledochus by biliary enteric anastomoses, sphincterotomy, stents, instrumentation, and portal bacteremia. Periampullary diverticula provide a site for bacterial proliferation with subsequent reflux into the bile duct (Fig. 43.2). Hemoglobinopathies may induce primary stones by providing a bilirubinate nidus for stone development. Foreign bodies including surgical clips and parasites may also introduce bacteria and serve as a nidus for stone formation, as shown in Fig. 43.3.3

Clinical Features and Diagnosis
The clinical presentation of biliary stones can be classified into three groups: (1) asymptomatic cholelithiasis or choledocholithiasis, (2) symptomatic gallstones (biliary colic), and (3) complications from gallstones (pancreatitis, cholecystitis, obstructive jaundice, cholangitis, gallbladder cancer, gallstone ileus). No symptoms occur in 60% to 80% of persons with gallstones, and the risk of progression is small. However, once symptoms develop, 35% to 50% of patients have recurrence within 1 year, and nearly 2% per year have complications.4
Biliary colic precedes complications in 90% of cases. The natural history of choledocholithiasis is unpredictable and not well described. Many common bile duct (CBD) stones are asymptomatic and pass into the duodenum without incident, whereas others lead to biliary colic, jaundice, cholangitis, or pancreatitis.5–7 Choledocholithiasis-associated biliary colic is similar to gallbladder-associated biliary colic. Untreated bile duct stone obstruction can cause secondary biliary cirrhosis, usually after about 5 years.8
Bile duct stones typically cause elevations in serum transaminases, alkaline phosphatase, and total bilirubin and ductal dilation on transabdominal ultrasound studies. However, CBD stones can be present with normal laboratory values. Total bilirubin levels range from normal to very high, and duration of obstruction does not correlate with serum bilirubin. Complete obstruction may cause a steady increase in serum bilirubin. Alkaline phosphatase is usually elevated up to fivefold in symptomatic patients. Acute biliary obstruction usually causes an initial disproportionate increase in transaminases.9
Imaging studies are the standard for the diagnosis of biliary stone disease. Transcutaneous abdominal ultrasound is the initial imaging study obtained when gallstone disease is suspected; sensitivity and specificity are greater than 95% for cholelithiasis and about 50% and 98% for bile duct stones.10 Spiral computed tomography (CT) is reported to be 82% sensitive and 97% specific for detecting bile duct stones, but many series have lower rates.11,12 Meta-analysis data show magnetic resonance cholangiopancreatography (MRCP) to be 92% sensitive and 97% specific for stones, but sensitivity declines for concretions 5 mm or less in diameter (Fig. 43.4).12,13

Fig. 43.4 Magnetic resonance cholangiopancreatography (MRCP) shows a 5-mm distal bile duct stone (arrow).
In a comparative study of 70 patients who underwent MRCP, transcutaneous ultrasound, or multislice CT, concordance was found between MRCP and ultrasound in 92% of cases for gallbladder lesions; however, statistically significant discordance occurred with ultrasound missing 16% of bile duct stones. Although there was concordance between MRCP and CT gallbladder imaging in 87% of patients, statistically significant discordance for bile duct lesions occurred in 35% of patients.14 Multiple studies show sensitivities and specificities for endoscopic retrograde cholangiopancreatography (ERCP) of 90% to 100% and 98% to 100%.12 Endoscopic ultrasound (EUS) can be performed with a dedicated echoendoscope with either 360-degree radial imaging or linear imaging or with an intraductal probe. EUS is performed similar to a standard endoscopy with ultrasound imaging of the extrahepatic bile duct done through the duodenal bulb or descending duodenum as shown in Fig. 43-5. Reported sensitivities and specificities for EUS are 84% to 100% and 96% to 100%.15

Preoperative diagnosis of CBD stones is not always necessary. Many authors advocate intraoperative cholangiography (IOC) as the diagnostic modality of choice in the setting of cholecystectomy with suspected CBD calculi. Laparoscopic IOC is technically successful in more than 90% of cases and is about 80% to 90% sensitive and 76% to 97% specific (Fig. 43.6).16,17 Fluoroscopic IOC has better diagnostic accuracy than static imaging. IOC is also used during cholecystectomy to verify biliary tree anatomy before dividing the cystic duct. IOC generally adds 5 to 25 minutes to the operation; however, it is usually faster, better tolerated, and less expensive than other invasive modalities.17 Laparoscopic intraoperative ultrasound is less widely employed than IOC. Yet, it has no radiation exposure, may be less time-consuming than IOC, and has sensitivity and specificity approaching 100%.17,18

Fig. 43.6 Intraoperative cholangiogram with two radiolucent stones seen in the common bile duct (CBD).
(Courtesy of Robert Glasgow, MD.)
Although 5% to 15% of persons who have cholecystectomy have bile duct stones, it is not cost-effective to perform universal IOC or ERCP, or both, for detection and treatment. Clinical, laboratory, and imaging studies are used to stratify for risk of harboring CBD stones. Numerous studies have identified risk factors and developed scoring formulas for risk. The most commonly detected factors are elevations in serum transaminases, alkaline phosphatase, and bilirubin, and bile duct dilation to 8 mm or larger on transabdominal ultrasound. However, only about 50% to 75% of persons predicted to be at high risk have choledocholithiasis.1,19,20 MRCP or EUS may be useful to define the risk more precisely; however, these tests add cost, and EUS-guided stone extraction is experimental.21 When stones are suspected preoperatively, the options for diagnosis and therapy are preoperative ERCP, IOC, and laparoscopic common duct exploration (LCDE). For stones detected by IOC and LCDE, intraoperative or postoperative ERCP can be done and obtain similar results. ERCP entails increased resource use, however.22 Conversion to open common duct exploration is associated with significant morbidity and prolonged hospital and recovery times, and open common duct exploration should not be used routinely. Choledocholithiasis may be diagnosed after surgery with transabdominal ultrasound, CT, MRCP, EUS, or ERCP, depending on the index of suspicion, and subsequently treated with ERCP.17
Biliary Sludge, Microlithiasis, and Crystals
Biliary sludge, microlithiasis, and crystals are a form of gallstone disease and seem to have a natural history and clinical associations similar to macroscopic stone disease. Over the course of 3 years, 50% of persons with abdominal pain and sludge have spontaneous resolution of the sludge, 20% have sludge with no symptoms, 10% to 15% have symptoms develop or persist, and 5% to 15% acquire stones. Sludge, microlithiasis, and crystals account for about 75% of cases of acute recurrent pancreatitis in which the etiology is undiagnosed by history, physical examination, blood tests, and noninvasive imaging studies.23–25 Cholesterol monohydrate crystals or calcium bilirubinate granules or both can be found in the gallbladder or bile duct after cholecystectomy in 67% to 89% of these patients.25–27 These lesions are also associated with cholelithiasis not seen on noninvasive imaging studies, cholecystitis without macroscopic stones, and cholangitis.
The initial diagnosis of gallbladder sludge is often made by transabdominal ultrasound, which has been reported to be 86% sensitive at showing a dependent layer of nonshadowing, slowly mobile material.28 MRCP is more sensitive than transabdominal ultrasound for the diagnosis of sludge and microlithiasis.29 EUS is about 96% sensitive for detecting sludge and finds small gallbladder and bile duct stones missed on other studies.28,30 Intraductal ultrasound probes are highly sensitive but may yield false-positive results. For lesions larger than 1.4 mm, intraductal ultrasound is 71% sensitive and 75% specific for microlithiasis validated by microscopy.31 Direct microscopic examination of the bile is considered the diagnostic standard, is more sensitive than transcutaneous ultrasound or EUS, allows the determination of the type of particles in the sludge, and is required to diagnose microlithiasis in the absence of sludge. However, crystals may occur intermittently, and false-positive and false-negative results may occur.2
Duodenal aspiration after stimulation of gallbladder emptying is cumbersome and yields a contaminated specimen. ERCP with gallbladder cannulation and aspiration provides a relatively pure specimen and has the added advantage of allowing for imaging of the biliary tree and pancreas and sphincter of Oddi manometry when indicated.32
Gallbladder bile (B bile) is opaque dark green or black and is much more informative than lighter colored hepatic bile (A bile) for diagnosing microlithiasis and crystals (Fig. 43.7). Some authors have collected dark bile with cannulation of only the choledochus, but this may be time-consuming and unsuccessful.33 Radiographic contrast material in the bile may cause false-positive microscopic examinations. I collect a pure bile specimen by gallbladder cannulation under fluoroscopic guidance before contrast injection into the gallbladder.

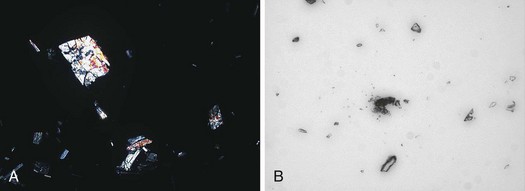
There is no consensus on the method of preparation, examination, and interpretation of bile specimens for microscopic crystal examination. Some authors have attempted to quantify the findings33; however, a qualitative examination is appropriate for clinical purposes.2 One suggested protocol is to centrifuge a 10- to 15-mL specimen at 3000g for 15 minutes and make a slide from the sediment. The slide is examined by light and polarizing microscopy at 100× (two crystals or granules per field or four per slide is considered a positive test). Cholesterol monohydrate crystals are rhomboid plaques with a notch that are multicolored on polarized examination, and bilirubinate granules are amorphous and red-brown colored as shown in Fig. 43.8. Leukocytes may be indicative of acute or chronic cholecystitis. It is difficult and unnecessary to maintain the specimen temperature strictly at 37° C, so the specimen should be centrifuged as quickly as possible. The intact specimen should not be stored because bacterial contamination can occur in specimens at room temperature and refrigerated specimens, and cholesterol crystal precipitation develops in frozen bile. However, the sediment may be frozen for later examination if necessary.2
Gallstone Pancreatitis
Gallstones cause about 35% of cases of acute pancreatitis in the United States, and about 25% of these cases are severe with mortality in 10%. Gallstones are recovered from the feces in 95% of patients with acute pancreatitis; however, only 7% of patients with gallstones develop pancreatitis.34 Soon after the onset of pancreatitis, 78% of affected persons have bile duct stones found at surgery or ERCP.35,36 However, delayed operations reveal CBD and impacted ampullary stones much less frequently.37
Small stones are thought to pass easily through the cystic duct and impact in the sphincter of Oddi; stones less than 5 mm in diameter are the most common.38 The causal relationship between gallstones and pancreatitis is confirmed by the finding that cholecystectomy or endoscopic sphincterotomy with removal of bile duct stones prevents recurrences.39 The pathophysiology may be due to obstruction of pancreatic juice outflow, reflux of offending substances into the pancreatic duct, or both.
The diagnosis of biliary pancreatitis is usually made by finding gallstones on transabdominal ultrasound in the absence of other known causes of pancreatitis, although EUS is more sensitive and specific and provides much better visualization of the bile duct.35 Abnormal liver enzymes and bilirubin and bile duct dilation on transabdominal ultrasound are frequently found but are nonspecific.40 It is important to stratify the severity of pancreatitis by various algorithms or failure of one or more organ systems because prognosis and therapy vary greatly between mild and severe cases. I use failure of one or more organ systems to categorize severe pancreatitis because algorithms are cumbersome and difficult to remember, include subjective criteria, and may require 48 hours of observation for a conclusion.41
Suppurative Cholangitis
Acute suppurative cholangitis develops in the setting of bacteria in the biliary system and bile duct obstruction. Bile duct stones are the cause of the obstruction in most cases. The bacteria enter the duct from the gut and proliferate resulting in increased intraductal pressure and forced translocation of bacteria and endotoxins into the hepatic sinusoids and bloodstream. In contrast to gallstone disease, women and men are affected equally with a median age of 50 to 60 years. Less frequently, benign and malignant strictures, obstructed stents, and side-to-side surgical anastomoses predispose to cholangitis. Mortality rates approach 100% in persons who fail conservative therapy and who do not have an adequate drainage procedure.42
The most common organisms are Escherichia coli, Enterococcus, Klebsiella, and Enterobacter. Pseudomonas, anaerobes, and skin and oral flora may be found after biliary instrumentation or surgery. Polymicrobial infection is more common in severe infections, and bile cultures are usually concordant.42 The classic clinical presentation is Charcot’s triad including fever, jaundice, and right upper quadrant abdominal pain; this occurs in 50% to 100% of patients. Reynold’s pentad adds altered mental status and hypotension to Charcot’s triad and occurs in less than 14% of patients. Typical laboratory abnormalities include leukocytosis, hyperbilirubinemia, elevated alkaline phosphatase, mildly increased transaminases, and occasionally elevated amylase.
Imaging findings on transabdominal ultrasound include stones or ductal dilation or both in 67% of patients. CT scans may show ductal dilation, the level of obstruction, and occasionally calcified CBD or gallstones or both. One study showed changes of papillitis to be 60% sensitive and 86% specific in homogeneous, hepatic contrast agent uptake to be 60% sensitive and 80% specific, and combined findings of papillitis and contrast agent uptake to be 97% specific for suppurative cholangitis.43 MRCP is reported to show distinctive changes in 92% of patients; however, because MRCP is without therapeutic capabilities, the utility is unclear. EUS may be beneficial in a clinically stable patient when ERCP is unsuccessful or undesirable because of increased procedure risks or pregnancy. Percutaneous transhepatic cholangiography (PTC) is sensitive and specific in 90% or more of affected patients and allows for therapy. However, it should not be considered as a first-line procedure because of high complication rates. ERCP is the procedure of choice because it affords the opportunity to provide diagnosis and definitive therapy with acceptable morbidity and mortality rates.
Treatment
Surgery
The management of CBD stones varies widely around the world. Therapeutic determinants include individual patient presentation; operative risk; and available expertise for LCDE, open CBD exploration, and ERCP. Laparoscopic cholecystectomy is the preferred initial approach to cholelithiasis with the benefit of decreased pain, shorter length of hospital stay, more rapid return to full activity, and less cost than open surgery. LCDE seems to have similar advantages over open CBD exploration and is cost-effective compared with ERCP.22 A transcystic duct approach is generally preferred to choledochotomy, resulting in shorter procedure duration and hospital stays and reduced need for T-tube placement. Some surgeons use a choledochotomy, however, depending on the stone. Stone extraction is generally achieved under fluoroscopic guidance with medical dilation of the sphincter of Oddi and flushing of small stones, by retrograde balloon or basket catheter techniques used to push stones through the native sphincter of Oddi, or after balloon dilation or antegrade sphincterotomy. Balloon dilation should be discouraged because of increased rates of pancreatitis. Choledochoscopic guidance may also be used with or without intracorporeal lithotripsy techniques.
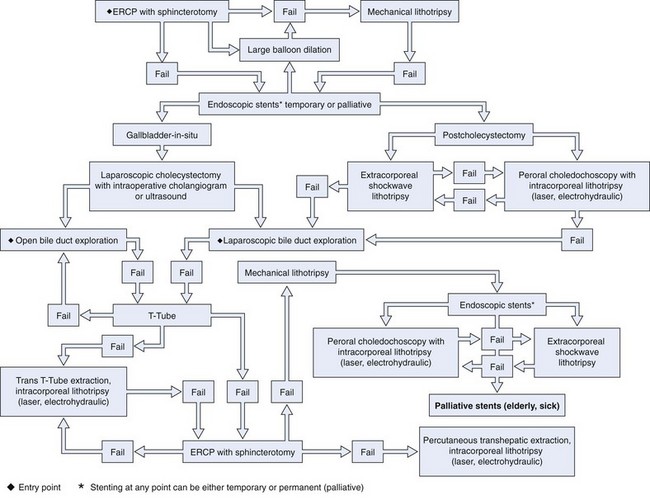
LCDE results in stone clearance in 75% to 90% of cases, and T-tube placement or antegrade biliary stent placement is required for incomplete drainage. LCDE adds about 1 hour to the operation. Transcystic duct LCDE requires hospital stays of about 1.5 days, and transductal procedures generally result in stays of up to 7.5 days. Morbidity and mortality rates are 10% and 1%.17 A treatment algorithm for preoperatively suspected bile duct stones managed by standard techniques is shown in Fig. 43.9. A treatment algorithm for bile duct stones requiring more specialized techniques is shown in Fig. 43.10. Stones detected after surgery are best managed by ERCP.
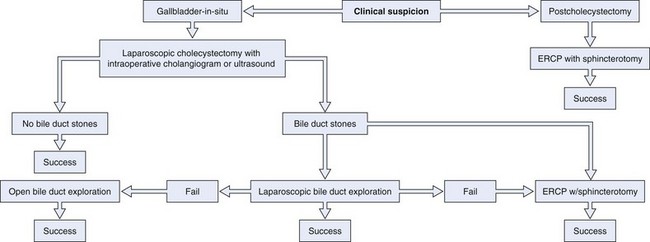
Fig. 43.9 Standard treatment for choledocholithiasis. ERCP, endoscopic retrograde cholangiopancreatography.
Endoscopic Therapy
ERCP with sphincterotomy is the most common method of treating bile duct stones in the United States, and more than 150,000 cases are performed each year. Overall, the procedure is ultimately successful in greater than 90% of patients with complications in about 10%.44 Successful clearance of the biliary tree of all stones depends on the size and number of stones and experience of the endoscopists. Reported rates of successful bile duct clearance range from about 60% to greater than 90% at the initial procedure45–48 to almost 100% with subsequent procedures at specialized centers.49–57 Failed cases are usually due to the inability to access the major papilla owing to surgically altered anatomy. Morbidity occurs in only 3% to 5% of patients from initial ERCP with sphincterotomy performed for stones, especially when performed within 30 days of laparoscopic cholecystectomy.48,58,59
Preoperative History and Considerations
Considerations in the medical history include prior intestinal surgery with altered anatomy such as Billroth or Roux-en-Y anastomoses, which could require a different approach and special instruments. Stones are common in pregnancy, and pregnancy could alter the timing and technique of ERCP. Preprocedure coagulation studies are not generally recommended but are appropriate in patients receiving anticoagulants or with biliary obstruction, who may develop a coagulopathy secondary to vitamin K malabsorption, which is significantly exacerbated in patients receiving warfarin. It is wise to have the international normalized ratio corrected to 1.5 or less if sphincterotomy is anticipated.60
Indications for general anesthesia include sepsis with hypotension; severe acute pancreatitis; significant cardiopulmonary disease; macroglossia; dysmorphic facies; obstructive sleep apnea; morbid obesity; and narcotic, benzodiazepine, or alcohol tolerance. Other considerations include a bowel purge in patients who have recently had a CT scan or other barium contrast study because residual barium in the colon can compromise cholangiography. Prophylactic antibiotics are not recommended for routine bile duct stone removal. However, antibiotics that cover enteric gram-negative organisms, enterococci, and perhaps Pseudomonas are recommended for cases of bile duct obstruction when there is a possibility of incomplete drainage.61
Therapeutic Techniques
Stones are extracted after cannulation has been achieved; the stone is identified on cholangiography, and the sphincterotomy is performed. A balloon or basket catheter is advanced upstream to the stone. The balloon is inflated and retracted, bringing the stone with it into the duodenum as shown in Fig. 43.11. A basket is positioned so that it completely opens and deploys such that the stone is totally engaged. It is often helpful to move or jiggle the basket gently up and down the affected segment of the duct to entrap the stone. The basket is left in the fully opened position and retracted into the duodenum, bringing the stone with it (Fig. 43.12). If the stone continually slips out of the basket, the basket may be closed around the stone to get a better grip. If this maneuver is done, it is important that the stone be small enough to pass through the distal duct and sphincterotomy orifice or that the basket be compatible with mechanical lithotripsy, to prevent basket and stone impaction in the duct. If multiple stones are present, the most downstream stone should be removed first also to prevent this type of impaction.

If the balloon or basket catheter is simply pulled out with the endoscope in the standard position, the stone is likely to be forced against the superior aspect of the duct deep to the duodenal wall. The catheter then slips out inferiorly to the stone. The balloon can rupture against the bridge on the endoscope, or the basket may slip off of the stone and out. Primary bile duct stones have an earthy consistency and crumble with extraction. It is often necessary to sweep the duct repeatedly with a balloon and perhaps irrigate the biliary tree with saline. Brown stone debris extracted into the duodenum is shown in Fig. 43.1C.
Unusual Situations
Pregnancy
About 8% of pregnant women develop cholelithiasis and frequently have symptoms. Cholecystectomy can often be postponed until after delivery; however, choledocholithiasis poses significant risk of cholangitis and pancreatitis and generally requires therapy. Potential risks to the fetus include sedatives and analgesics; radiation exposure; and sequelae of procedural complications such as hypoxia, pancreatitis, and sepsis. There are several small series in the literature of ERCP during pregnancy including during the first trimester. Biliary sphincterotomy, stone extraction, and stent placement were frequently done. Most patients delivered healthy full-term infants. Therapeutic outcomes were generally successful with acceptable morbidity.62
A reasonable approach is to perform transabdominal ultrasound for pregnant women who develop right upper quadrant or epigastric pain, abnormal serum hepatic enzymes, unexplained acute pancreatitis, or biliary sepsis. If gallstones are found and there is no pancreatitis, cholecystectomy may be postponed until after delivery if the symptoms and biochemical tests resolve.62 ERCP is indicated for choledocholithiasis or ductal dilation seen on ultrasound, persistent cholestasis, pancreatitis, or cholangitis. The patient should be considered for referral to a high-volume center with experience in these cases. Obstetric consultation should be obtained, and fetal monitoring should be considered during the procedure. The procedure may need to be performed in the supine or left lateral position. It may be wise to have an anesthesiologist administer the sedation or anesthesia and to consider endotracheal intubation if the patient is to be in the supine position.
Fetal radiation exposure should be minimized by lead shielding; using minimal fluoroscopy; and avoiding spot films, which give higher radiation exposure. Using these techniques, fetal radiation exposure can be contained to about 310 mrad, which is significantly below the accepted teratogenic dose.63 Radiation exposure to the fetus may be monitored with a radiation dosimetry badge placed on the mother’s abdomen over the uterine fundus.
Sphincterotomy and stent placement may be safely performed, and transpapillary gallbladder stent placement for cholecystitis has been suggested to postpone cholecystectomy until after delivery.62,64 Some authorities advocate performing the procedure with no fluoroscopy. One technique is to use wire-guided cannulation with visualization of bile flow around the wire, through a small-caliber stent, or with aspiration through the sphincterotome. Sphincterotomy may be performed in the standard fashion or with a needle-knife over a stent. Stones can be removed with balloons, baskets, or mechanical lithotripsy.65 Alternatively, a stent may be left in situ, and ERCP may be repeated after delivery.66 Cholangioscopy has been used to confirm ductal clearance.67 Ultrasound, rather than fluoroscopic, guidance has also been used.
Biliary Sludge, Microlithiasis, and Crystals
Traditional therapy for sludge, microlithiasis, and crystals is cholecystectomy, which generally cures relapsing pain and prevents recurrent pancreatitis. Ursodeoxycholic acid can dissolve cholesterol microlithiasis and crystals and prevents the recurrence of pancreatitis. However, the duration of effect is unknown.2 Endoscopic sphincterotomy prevents or reduces episodes of recurrent pancreatitis caused by sludge, microlithiasis, and crystals.33
Gallstone Pancreatitis
The usual therapy for mild to moderate disease is supportive until pancreatitis resolves and then laparoscopic cholecystectomy with IOC generally during the same hospital stay. Severe disease is best treated with intensive care monitoring, prophylactic antibiotics for extensive necrosis, enteral nutritional support, and urgent biliary drainage for signs of bile duct obstruction (jaundice, persistently abnormal liver tests, and dilated bile duct) or cholangitis. Early biliary surgery is associated with high rates of morbidity and mortality in severe pancreatitis.36 Cholecystectomy should be performed during the same hospital stay or as soon as possible afterward.
Urgent endoscopic retrograde cholangiography (ERC) with biliary sphincterotomy and stone extraction has been used to reduce morbidity and mortality.68 There are six published peer-reviewed, randomized controlled trials of ERC compared with conservative management in patients with acute pancreatitis, and there are six meta-analyses of these studies with conflicting results. The conflicting results are due to heterogeneity of patients, inclusion criteria, severity of disease, and inability to confirm the presence of stones. There are also different methodologies and endpoints.68–79 Extraction of obstructing stones is beneficial in relieving cholangitis and jaundice. There are several issues pertinent to interpreting this literature, as follows: (1) Does ERC prevent systemic or pancreatic morbidity? (2) Should ERC be done in all cases or only for cholangitis or biliary obstruction? (3) Is it beneficial to diagnose CBD stones with noninvasive imaging or EUS and then do ERC only if stones are seen? (4) Should sphincterotomy be done in all patients to provide drainage for unseen microlithiasis, sludge, or stones? (5) What is the optimal timing for ERCP?
Neoptolemos and colleagues69 randomly assigned 121 patients from a single center with suspected biliary pancreatitis to have ERC with sphincterotomy for bile duct stones within 72 hours of admission compared with conservative therapy. Subgroup analysis of patients with severe pancreatitis showed a statistically significant decrease in morbidity and a numerical benefit in mortality. Fan and coworkers70 randomly assigned 195 patients with pancreatitis of any etiology (including alcohol and hyperlipidemia) to receive ERC with sphincterotomy for choledocholithiasis within 24 hours of hospitalization or medical management. The overall outcomes were similar for the treatment and control groups; however, in patients with severe pancreatitis, morbidity was significantly less frequent at 13% versus 54% (P = .003). There was a trend toward improved mortality rates in the ERC group at 3% versus 18% (P = .097). Biliary sepsis occurred less commonly in patients with severe disease treated with ERC than conservative management at zero and 29% (P < .001). Issues with this study are inclusion of patients with pancreatitis of all causes and patients with cholangitis.
In a multicenter German study, 238 subjects were randomly assigned to ERC with sphincterotomy and stone extraction within 72 hours of symptom onset or conservative management. Patients with cholangitis or a total bilirubin of 5 mg/dL or greater were excluded. Of 112 patients randomly assigned to conservative management, 20 went on to ERC, and 13 had stones extracted. The overall morbidity rates were similar between the ERC and control groups, but the data were not stratified by severity of pancreatitis. There were more serious complications in the treatment group, mostly because of respiratory failure (P = .03), but fewer episodes of cholangitis. Death occurred in 14 treatment and 7 control patients; most deaths were due to respiratory failure. Pancreatic morbidity rates were similar between the groups at 23% and 22%. The authors concluded that early ERC with sphincterotomy is not beneficial in patients with acute biliary pancreatitis and no obstructive jaundice or cholangitis. Problems with this study were that there were significantly fewer patients with stones and severe disease than in the other studies and that 19 of the 22 centers enrolled fewer than two subjects per year on average. The rate of respiratory failure in the ERC group was higher than in other studies. Considering the low volume at some centers and the undue rates of respiratory failure, questions have been raised about the degree of endoscopic expertise and potential for procedure-related aspiration.71
Zhou and colleagues72 randomly assigned 45 patients with gallstone pancreatitis stratified by severity to have ERC within 24 hours or medical therapy. Sphincterotomy and extraction was done for small stones, and nasobiliary drainage was performed for large or no stones. Morbidity and length of hospitalization were significantly decreased in severe cases with ERC but not for mild disease. Issues with this study include the small sample size and that cholangitis was not explicitly excluded.
Another more recent randomized trial included 61 patients with gallstone pancreatitis and ampullary obstruction assigned to a control group of conservative therapy with selective ERC at 48 hours or a treatment group with ERC at 24 hours for persistent obstruction. In 9 of 31 control patients, obstruction did not spontaneously resolve, and 3 had ERC and sphincterotomy with no stones found. Among the treatment patients, obstruction resolved in 16, and 11 of 14 who had ERCP had stones removed. There was a statistically significant lower morbidity rate in the treatment group, and the authors concluded that these patients should have ERC within 48 hours. However, only 47% of the treatment patients had ERC.73
Oria and colleagues74 randomly assigned 103 patients with acute gallstone pancreatitis with elevated bilirubin and dilated bile ducts but no cholangitis to ERC with sphincterotomy for stones or conservative management, and outcomes were stratified by severity. Bile duct stones were detected in 72% of the ERC group and 42% of the conservative group at subsequent surgery. There were no statistically significant differences between the groups in morbidity, CT index, local complications, or mortality. Limitations of the study are the small sample size and inclusion of patients with mild to moderate disease.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


