Chapter 5 Autoimmune hepatitis
Definition
TABLE 5.1 Autoimmune hepatitis: Basic diagnostic tests
| Diagnostic tests | Clinical value |
|---|---|
| Serum AST and ALT, bilirubin, alkaline phosphatase, and γ-globulin levels | Estimate severity of inflammatory activity; characterize pattern of liver injury |
| Serum albumin level and INR | Estimate impairment of hepatic synthetic function |
| ANA, SMA, anti-LKM1, and AMA | Document presence and nature of immune activity |
| Serum immunoglobulin levels | Confirm mainly serum IgG elevation |
| Liver tissue examination | Document that histologic changes support diagnosis Exclude findings suggestive of other diagnoses |
| HBsAg, anti-HBc, IgM anti-HAV, and anti-HCV | Document absence of concurrent viral infection |
| Ceruloplasmin level | Exclude Wilson disease |
| Alpha-1 antitrypsin phenotype | Exclude alpha-1 antitrypsin deficiency |
| Serum iron, transferrin, iron saturation and ferritin levels | Exclude hereditary hemochromatosis |
AMA, antimitochondrial antibodies; ANA, antinuclear antibodies; anti-HAV, antibody to hepatitis A virus; anti-HBc, antibody to hepatitis B core antigen; anti-HCV, antibody to hepatitis C virus; anti-LKM1, antibodies to liver kidney microsome type 1; AST, aspartate aminotransferase; ALT, alanine aminotransferase; HBsAg, hepatitis B surface antigen; IgG, immunoglobulin G; INR, international normalized ratio; SMA, smooth muscle antibodies.
Nomenclature
Diagnosis
TABLE 5.2 International criteria for definite or probable diagnosis of autoimmune hepatitis
| Diagnostic features | Definite diagnosis | Probable diagnosis |
|---|---|---|
| Exclusion of risk factors for other diseases | ||
| Inflammatory indices | ||
| Autoantibodies | ANA, SMA, or anti-LKM1 >1:80 in adults and >1:20 in children; no AMA | ANA, SMA or anti-LKM1>1:40 in adults; other autoantibodies |
| Immunoglobulins | Globulin, γ-globulin, or IgG level >1.5 times normal | Hypergammaglobulinemia of any degree |
| Histologic findings |
AMA, antimitochondrial antibodies; ANA, antinuclear antibodies; AT, antitrypsin; anti-LKM1, antibodies to liver kidney microsome type 1; AST, aspartate aminotransferase; ALT, alanine aminotransferase; IgG, immunoglobulin G; SMA, smooth muscle antibodies.
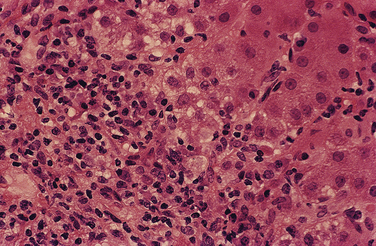
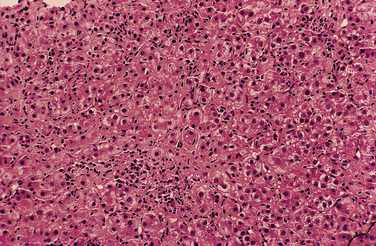
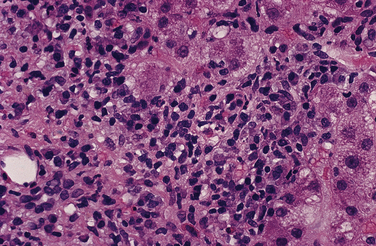
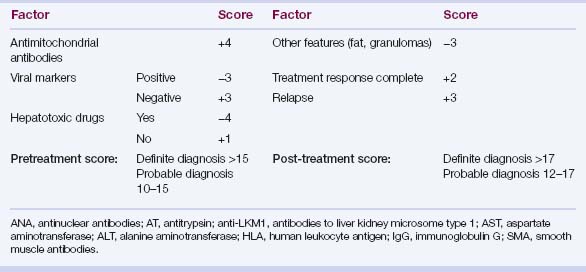
TABLE 5.4 Simplified international scoring system for the diagnosis of autoimmune hepatitis
| Variable | Result | Points |
|---|---|---|
| Autoantibodies | ||
| ANA or SMA | ≥1:40 | +1 |
| ANA or SMA | ≥1:80 | +2 |
| anti-LKM1 | ≥1:40 | +2 |
| anti-SLA | Positive | +2 |
| Immunoglobulin level | ||
| Immunoglobulin G | >ULN | +1 |
| >1.1 ULN | +2 | |
| Histologic findings | ||
| Morphologic features | Compatible | +1 |
| Typical | +2 | |
| Viral disease markers | ||
| No viral hepatitis | No viral markers | +2 |
| Pretreatment aggregate score: | ||
| Definite diagnosis | ≥7 | |
| Probable diagnosis | 6 | |
ANA, antinuclear antibodies; anti-LKM1, antibodies to liver kidney microsome type 1; anti-SLA, antibodies to soluble liver antigen; SMA, smooth muscle antibodies; ULN, upper limit of normal.
Pathogenesis
Principal hypotheses
 A triggering viral, drug, toxic, or environmental agent that resembles a self-antigen (molecular mimicry)
A triggering viral, drug, toxic, or environmental agent that resembles a self-antigen (molecular mimicry)
 A six amino acid motif within an antigen binding groove, encoded as LLEQKR (leucine-leucine-glutamic acid-glutamine-lysine-arginine) in positions 67 to 72 of the DRβ polypeptide chain, that optimizes autoantigen display in white North American and northern European patients
A six amino acid motif within an antigen binding groove, encoded as LLEQKR (leucine-leucine-glutamic acid-glutamine-lysine-arginine) in positions 67 to 72 of the DRβ polypeptide chain, that optimizes autoantigen display in white North American and northern European patients











Ancillary hypotheses
 Different susceptibility alleles encode the same or similar six amino acid motif within the antigen binding groove of the HLA DR molecule between positions 67 and 72 of the DRβ polypeptide chain and thereby affect susceptibility similarly.
Different susceptibility alleles encode the same or similar six amino acid motif within the antigen binding groove of the HLA DR molecule between positions 67 and 72 of the DRβ polypeptide chain and thereby affect susceptibility similarly.

 Polymorphisms of genes inside and outside the major histocompatibility complex act in synergy with each other or the principal susceptibility alleles in a non–disease-specific fashion to promote susceptibility (“permissive gene pool”).
Polymorphisms of genes inside and outside the major histocompatibility complex act in synergy with each other or the principal susceptibility alleles in a non–disease-specific fashion to promote susceptibility (“permissive gene pool”).





Subclassifications
Types


























Variants
 Defined by features of autoimmune hepatitis, antimitochondrial antibodies (AMA), and histologic findings of bile duct injury or loss
Defined by features of autoimmune hepatitis, antimitochondrial antibodies (AMA), and histologic findings of bile duct injury or loss Most (88%) patients with AMA titers up to 1:160; seropositivity for antibodies to M2 autoantigens rare (8%) (see Chapter 14)
Most (88%) patients with AMA titers up to 1:160; seropositivity for antibodies to M2 autoantigens rare (8%) (see Chapter 14)


 Defined by features of autoimmune hepatitis, cholestatic biochemical changes, histologic evidence of cholestasis including bile duct injury or loss, and abnormal bile ducts by endoscopic retrograde cholangiography (ERC) or magnetic resonance cholangiography (MRC)
Defined by features of autoimmune hepatitis, cholestatic biochemical changes, histologic evidence of cholestasis including bile duct injury or loss, and abnormal bile ducts by endoscopic retrograde cholangiography (ERC) or magnetic resonance cholangiography (MRC)





 SMA and ANA titers typically low in chronic viral hepatitis (up to 1:80 in 89%, 1:160 or higher in 11%; 1:320 or higher rarely)
SMA and ANA titers typically low in chronic viral hepatitis (up to 1:80 in 89%, 1:160 or higher in 11%; 1:320 or higher rarely)



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


