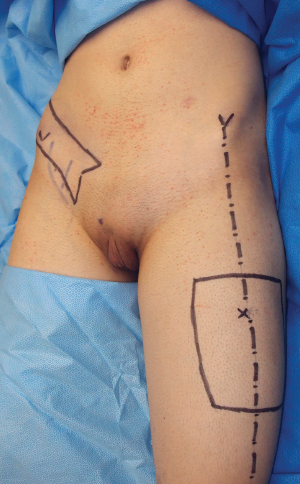
CHAPTER 9 The anterolateral thigh (ALT) flap was introduced as an alternative flap for phalloplasty in 2006 by Felici and Felici1 as a free flap and by Mutaf et al2 as a pedicled flap. Since then, 52 cases have been published to date,3–13 of which the largest series was 13 cases.14 The ALT flap phalloplasty was introduced as an alternative to the standard phalloplasty technique: the radial forearm flap (RFF). The RFF is considered the method of choice for several reasons: 1. No other flap has been used so extensively in phalloplasty; the RFF is the only flap that has been proved effective and safe in large series.14,15 2. It is thin and pliable enough to allow a tube-within-a-tube reconstruction of a (skin-lined) urethra with one flap, and even in large series patients managed to void while standing in all cases.14 3. At least two sensory nerves can be included in the flap, and sensory innervation is of good quality. 4. It effectively accommodates an erectile prosthesis, making satisfactory sexual intercourse possible.16 5. The flap can be easily shaped to reproduce a penis. 6. Morbidity is acceptable.17 Despite all these advantages, there are reasons to look for an alternative technique. Phalloplasty with an RFF is a microsurgical operation that requires close postoperative monitoring and potentially necessitates anastomotic revision, increasing the workload of an already complex surgery. Furthermore, skin grafting of the donor site—covering a large part of the forearm—is a well-known stigmata of the surgery that not all patients are willing to accept. To avoid a forearm scar, many alternative techniques for phalloplasty have been described. Sporadic reports with other types of free flaps such as the fibula flap,18–21 the latissimus dorsi,22 the deltoid flap,23 and the thoracodorsal artery perforator flap24 can be found in the literature. All these flaps share some common drawbacks: The only theoretical advantage of these other free flaps is the absence of the forearm scar, but because the goal of surgery is to reconstruct a penis that is as functional and aesthetic as possible, these various techniques thus far have not met either the standards or the quality of an RFF phalloplasty. Furthermore, the complexity of the procedure is not reduced, because these are also microsurgical techniques. To avoid the additional complexity of a microsurgical procedure, pedicled flap phalloplasties have also been described with the use of abdominal skin,25 groin flaps,26 or gracilis flaps.27 However, these techniques also share some of the previously mentioned drawbacks regarding urethral reconstruction, decreased or absent sensation, less aesthetic appearance, and a small nonstandardized series. Taking all these factors into consideration, the ideal alternative to the RFF phalloplasty should have the following characteristics: The ALT flap seems a promising alternative to the RFF because: Although it has all these positive qualities, the ALT phalloplasty has not gained popularity so far, and at best only sporadic case reports or small series can be found in the literature. The main reason is that urethral reconstruction in an ALT phalloplasty is not easy to accomplish, because the flap is seldom thin enough to reconstruct it with the tube-within-a-tube technique. Only a few case reports have been published on how to solve this problem, and most only have a short follow-up or report unclear outcomes regarding urinary function.1–13 How to efficiently reconstruct the urethra when using an ALT flap is still unclear, and this has greatly limited its application to patients in whom urethral reconstruction was not needed, such as patients with bladder exstrophy. These patients usually have a permanent urinary diversion. When these patients need urethral reconstruction, which are typically young male patients, the subcutaneous fatty layer of the thigh is often thin enough to allow a urethral reconstruction with the tube-within-a-tube technique. Unfortunately, these patients are only a small number of those seeking phalloplasties, because fortunately bladder exstrophy is quite rare. The largest demand for phalloplasty is from female-to-male transsexual patients seeking sex reassignment surgery (SRS). The difference between these patients and biologic males seeking phallic reconstruction after bladder exstrophy or amputation is that female-to-male patients have withstood the influence of female hormones; these patients have a gynoid habitus with thicker thighs. In this patient population urethral reconstruction with the tube-within-a-tube technique is almost never possible with an ALT flap because of excess flap thickness. The first report of the lateral thigh as a donor site for phalloplasty was that of Santanelli and Scuderi,28 who used a pedicled tensor fasciae latae (TFL) flap. Urethral reconstruction was accomplished in three stages by (1) flap prelamination, (2) tissue expansion at the second stage, and (3) finally flap transfer with tubing of the urethra. The outcomes of urethral reconstruction were unclear, and eventually only one patient maintained the reconstructed urethra after 2 years. This technique has been used in five cases, and no further reports can be found in the literature afterward. The reconstructed phallus lacked a glans and corona, and thus although functionally acceptable, cosmetically it was not ideal. Furthermore, the flap needed defatting of the pedicle in the groin, adding up to a total of four procedures. Another increasing patient group are those who have previously undergone a phalloplasty with or without urethral reconstruction and again request penile reconstruction of a shriveled penis or after an inadequate phalloplasty. These patients can be ideal candidates for an ALT phalloplasty. The ALT phalloplasty seems the most promising alternative to the free RFF if an effective way for urethral reconstruction is found. In this chapter we will describe the technique of ALT flap phalloplasty and the different methods for reconstructing the urethra to accomplish an aesthetic and a functional penile construction. The ALT flap is named based on its nourishing artery, the descending branch of the lateral circumflex femoral artery (DBLCFA) perforator flap.29 Flaps such as the TFL perforator flap can be harvested from the ALT, thus confusing the nomenclature. However, for the purpose of simplicity and adherence to the most commonly used nomenclature, the DBLCFA perforator flap will still be referred to as the ALT flap. Perforators to the ALT flap originate at various distances from the DBLCFA, which travels in the septum between the vastus lateralis and rectus femoris muscles and then lies on the medial margin of the vastus lateralis,30,31 in close proximity to the motor nerve to the vastus lateralis. It gives off, early after its origin, one or two short branches that nourish the rectus femoris and cross its motor nerve. The anatomy of the DBLCFA perforators can vary considerably; they are most frequently found in the middle third of the thigh, just lateral to the intermuscular septum. Myocutaneous perforators are more commonly encountered than septocutaneous perforators. The position of the perforator and its course influence pedicle length: the more distal and lateral the perforator, the longer the pedicle. A septocutaneous perforator warrants a faster dissection, because it avoids intramuscular dissection, ligation of several intramuscular branches, and identification and preservation of small intramuscular motor nerves. With free flaps the position of the perforator has little influence, because pedicle length has lesser importance, and a suitable perforator can always be found by eventually switching to an anteromedial thigh flap32 or a TFL flap33 if no suitable “ALT” perforator is found. When a pedicled flap is planned that should reach the pubic area, pedicle length becomes of paramount importance. Because perforator anatomy is unpredictable, accurate preoperative perforator localization is mandatory to plan these flaps. Sensory nerves to the lateral thigh skin come from the lateral femoral cutaneous nerve, and like anywhere else in the body, they constantly run across the largest perforators that nourish them on their course to the skin. This implies that in a conventional freestyle ALT flap, the nerves can guide the surgeon to the best perforator; in an ALT flap phalloplasty, in which the best perforator is determined before surgery by CT angiography, the nerves will be found running close to the perforator. The main nerve branches usually run in the loose plane between the fascia and subscarpal fat and are accompanied by large perineural vessels, branches of the perforator, throughout their whole length.34 Sometimes only one large nerve is found. In these cases the two fascicles of the nerve are separated to obtain two branches for nerve coaptation. The skin of the ALT is thicker than that of the forearm. The skin usually has hair, and mainly the subcutaneous fat is much thicker and divided in two layers by Scarpa fascia; several vertical septa are needed to hold the skin and fat against gravity, making it more rigid and less pliable compared with a forearm flap. There are various perforators nourishing the lateral thigh skin coming from the DBLCFA that travel either through the muscle or septum and reach the skin at different levels on the thigh. As previously mentioned, their position is unpredictable. With a free flap, a retrograde freestyle approach can be used.35 After simple preoperative Doppler localization, the perforators are identified through an exploratory incision; the best one is chosen during surgery and further dissected out until its source vessel is reached. The dissection of an ALT free flap does not require preoperative knowledge of the best perforator, which side has the best perforator, which perforator is septocutaneous, and pedicle length, but with a pedicled flap, all these details are fundamental. In pedicled ALT flap phalloplasty, this freestyle retrograde approach, in which there is no information on position, course, and pedicle length of the perforator, is not advisable, because there is a risk that the wrong side was chosen, the best perforator or a septocutaneous perforator was missed, or eventually the pedicle is too short. Preoperative CT angiography is needed to investigate perforator anatomy of both thighs to identify the “best” perforator, which is a big perforator (not necessarily the biggest), long enough to comfortably reach the pubic area without undue traction, and preferably a septocutaneous perforator or one with a short intramuscular course. Furthermore, as mentioned previously, the accurate choice of the perforators guarantees that the sensory nerves lie in close proximity. We have started using a CT scan after we encountered problems in a patient in whom, after preoperative tissue expansion of the thigh at the time of surgery, we found no perforators to harvest an ALT. We had to stop the operation and change the surgical plan; we performed an RFF phalloplasty 2 weeks later. The additional benefit of CT angiography is that it also allows measurement of flap thickness to estimate the circumference of the neophallus and subsequently the required flap dimensions. Preoperative perforator location becomes especially useful when preoperative expansion with a medial and lateral expander is planned. In these cases an exact location of the best-suited perforator is an absolute requirement. Recently noncontrast MRI has been introduced for preoperative perforator mapping.36 The point where the perforator pierces the fascia will be measured starting from the line connecting the anterior superior iliac spine (ASIS) and the upper lateral angle of the patella. This line corresponds to the septum between the rectus femoris and vastus lateralis muscles. No specific patient preparation is needed for the actual phalloplasty. Preoperative CT angiography is absolutely necessary for perforator location, as discussed previously, and is obtained before surgery for two reasons: 1. Complete flap epilation is ideally completed before surgery. If this is not possible, at least the urethral part (for tube-within-a-tube phalloplasties) of the flap will be hairless. When urethral reconstruction is not planned, the outer part of the flap can undergo definitive epilation after surgery. The part that must undergo epilation can be decided only after the perforator is chosen with the CT scan. 2. If preoperative expansion is planned to avoid skin grafting of the donor site, CT angiography is performed first to locate the perforator. Two expanders are then placed in the suprafascial plane at the lateral and medial borders of the flap. The skin lateral and medial to the flap, not the actual flap, is expanded so that the flap and the perforator are not affected by expansion. To accomplish this, the surgeon must know the exact perforator location and flap size based on the measurements obtained from the CT angiogram. Perioperative antibiotic prophylaxis is administered starting on the day of surgery.37 The ASIS is marked on the chosen side, and a line is drawn that connects it to the upper lateral angle of the patella. The position of the perforator is marked precisely on the thigh skin based on the X and Y coordinates provided by the CT scan, and the flap is drawn around it with the perforator lying along its midline axis and close to its proximal border (Fig. 9-1). The length of the flap is usually 14 cm. The width is determined based on flap thickness as measured on the CT scan. Because the reconstructed phallus can be considered a cylinder, with its cross-section a circumference, the estimated outer circumference, which corresponds to the transverse axis of the flap, can be calculated with the following formula: 2πr, where r corresponds to thickness of the ALT flap in millimeters as measured on the CT scan plus the thickness of the planned urethra in millimeters plus 5 (this latter to compensate for the presence of the urinary catheter and postoperative edema). This means that a 20 mm thick ALT combined with a 5 mm thick superficial circumflex iliac artery perforator (SCIAP) (see Fig. 9-1) will be 2 × 3.14 × (20 + 5 + 5) = 188.4 mm wide. If these rules are not respected, closure may be too tight, and a ventral skin graft will be needed to avoid flap compression. It is not infrequent that the flap is wider than it is long. This can potentially mislead the surgeon, who may tend to think that the longer side is the longitudinal axis, thus causing rotation and malpositioning of the flap. The nerves always allow correct flap orientation, because they always enter the flap from the proximal side.
Anterolateral Thigh Flap Phalloplasty
Key Points
 A pedicled anterolateral thigh flap can be a valuable alternative to a radial forearm flap phalloplasty to avoid the typical scar in the forearm.
A pedicled anterolateral thigh flap can be a valuable alternative to a radial forearm flap phalloplasty to avoid the typical scar in the forearm.
 The flap is planned with the aid of preoperative CT angiography to locate the best perforator.
The flap is planned with the aid of preoperative CT angiography to locate the best perforator.
 Two nerves are always taken with the flap. One is sutured to an ilioinguinal nerve for restoration of protective sensation, and the other is sutured to one of the dorsal clitoral nerves.
Two nerves are always taken with the flap. One is sutured to an ilioinguinal nerve for restoration of protective sensation, and the other is sutured to one of the dorsal clitoral nerves.
 The flap is tunneled underneath the rectus femoris and sartorius muscles and then subcutaneously to reach the pubis. In rare cases a short pedicle makes conversion to a free flap necessary.
The flap is tunneled underneath the rectus femoris and sartorius muscles and then subcutaneously to reach the pubis. In rare cases a short pedicle makes conversion to a free flap necessary.
 Urethral reconstruction can rarely be accomplished with the same flap, because the thigh fat is too thick most of the time. A second skin flap is the best way to reconstruct the urethra.
Urethral reconstruction can rarely be accomplished with the same flap, because the thigh fat is too thick most of the time. A second skin flap is the best way to reconstruct the urethra.
 A free radial forearm flap and pedicled superficial circumflex iliac artery perforator are the methods of choice for urethral reconstruction.
A free radial forearm flap and pedicled superficial circumflex iliac artery perforator are the methods of choice for urethral reconstruction.
 Urethral reconstruction is not performed or achieved with multiple flaps or skin/mucosal grafts, which increase the risk of strictures and fistulas.
Urethral reconstruction is not performed or achieved with multiple flaps or skin/mucosal grafts, which increase the risk of strictures and fistulas.
 Sensation is rarely restored or is of low quality, making implantation of an erectile prosthesis less safe.
Sensation is rarely restored or is of low quality, making implantation of an erectile prosthesis less safe.
 It is difficult to shape the neophallus appropriately.
It is difficult to shape the neophallus appropriately.
 Only small series are published, and subsequently the techniques cannot be standardized.
Only small series are published, and subsequently the techniques cannot be standardized.
 Be safe and reliable
Be safe and reliable
 Allow reconstruction of an aesthetically acceptable phallus
Allow reconstruction of an aesthetically acceptable phallus
 Allow reconstruction of a competent penile urethra with a single tube, minimizing risks of strictures and fistulas so that patients are able to void while standing
Allow reconstruction of a competent penile urethra with a single tube, minimizing risks of strictures and fistulas so that patients are able to void while standing
 Be sensate and allow implantation of an erectile prostheses to have satisfactory sexual intercourse
Be sensate and allow implantation of an erectile prostheses to have satisfactory sexual intercourse
 Be pedicled to reduce the complexity of a free flap phalloplasty
Be pedicled to reduce the complexity of a free flap phalloplasty
 Have an acceptable or better concealed donor-site scar
Have an acceptable or better concealed donor-site scar
 It is one of the most commonly used flaps and is safe and reliable.
It is one of the most commonly used flaps and is safe and reliable.
 It can be shaped into an acceptable phallus.
It can be shaped into an acceptable phallus.
 It can be reinnervated by branches of the lateral femoral cutaneous nerve.
It can be reinnervated by branches of the lateral femoral cutaneous nerve.
 It lies close to the recipient site and can subsequently be used as a pedicled flap.
It lies close to the recipient site and can subsequently be used as a pedicled flap.
 The donor site can be concealed under men’s clothing.
The donor site can be concealed under men’s clothing.
Anatomy
Preoperative Planning
Patient Preparation
Preoperative Markings
Abdominal Key
Fastest Abdominal Insight Engine