Chapter 21 ANAL PAIN
CAUSES OF ANAL PAIN
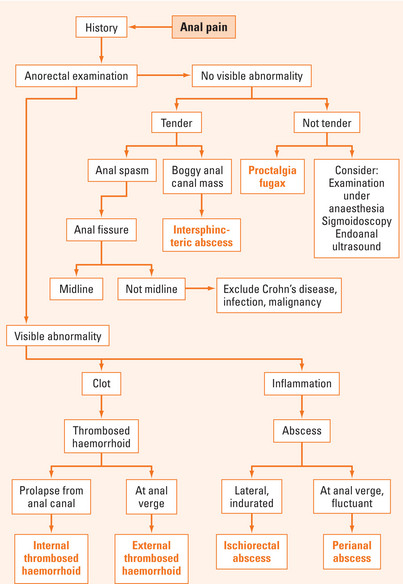
There are many causes of anal pain (Table 21.1). Patients usually attribute anal pain to haemorrhoids. However, haemorrhoids rarely cause pain unless they are complicated by prolapse and thrombosis. There is usually some delay in presentation because of patient embarrassment. A thorough history and careful examination can usually elicit the diagnosis without need for further investigations (Figure 21.1). Occasionally, other investigations are required and may include examination under anaesthesia, biopsy and pathological analysis, sigmoidoscopy, endoanal ultrasound and magnetic resonance imaging (MRI).
TABLE 21.1 Causes of anal pain
| Frequency | Causes |
| Common | |
| Infrequent | |
| Rare | • Anal tumours (squamous cell carcinoma, melanoma, Bowen’s disease, Paget’s disease, basal cell carcinoma) |
Anal fissure
Anal fissure is caused by a tear in the mucosa of the anal canal, usually from a hard stool. It causes anal pain worse on defecation, lasting for several hours and associated with a small amount of bright red rectal bleeding. Physical examination may reveal the triad of internal anal papilloma, anal fissure and external sentinel skin tag. Sphincter muscle is present in the base of the fissure. Of all anal fissures, 90% are located in the posterior region, 5% in the anterior region and 5% in other areas. When an anal fissure is not situated in the posterior or anterior positions, a secondary aetiological factor (e.g. Crohn’s disease, infection or malignancy) should be entertained. Delay in healing of anal fissures has been attributed to impaired blood supply, demonstrated on ultrasound Doppler studies and postmortem studies.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


