evaluating the sensitivity and specificity of CTC using multidetector row CT. Multidetector computed tomography (MDCT) allows for thinner collimation of 1.25 mm or smaller. This may lead to improved spatial resolution and increased sensitivity, particularly for smaller polyps and flat lesions. Additionally, narrower collimation may allow easier differentiation between a true polyp versus stool so that there are fewer false positives, leading to increased specificity. However, the use of thinner collimation includes drawbacks such as higher effective radiation dose to the patient, noisier images, and larger data sets for evaluation and storage.
TABLE 7.1 Polyp Detection: Single-Center Studies | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
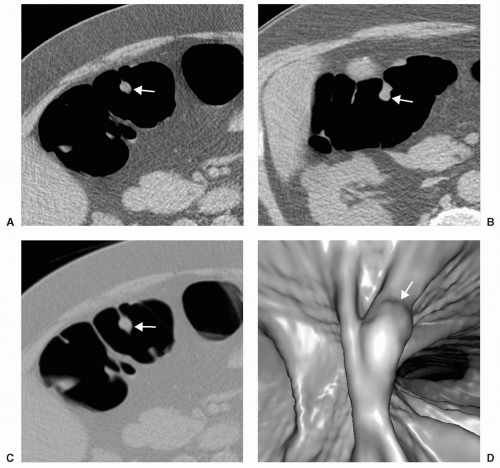 FIGURE 7.1 Large Polyp in an Asymptomatic Screening Patient. A large polyp is visualized on the axial images in abdominal window in both supine (A) and prone (B) images. The appearance of the lesion is more prominent using a colon window (C). The lesion was also identified on the 3D endoluminal view (D). |
provide rapid differentiation of a polyp from a fold and is the preferred interpretation technique by some readers because it may be easier to learn and identify polyps. Primary 3D interpretation has been found in several published studies to be an accurate visualization technique for lesion detection.3,13
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


