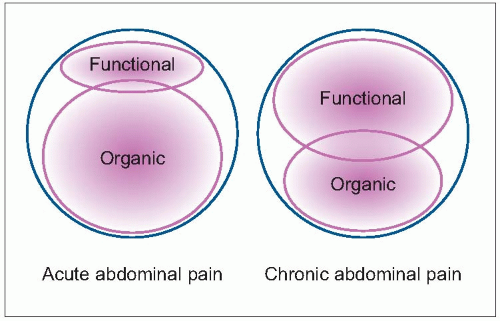
Abdominal pain is one of the most challenging symptoms in paediatric practice. Often imprecise, abdominal pain may require, especially if acute, an intense diagnostic approach in order to avoid misidentification of potentially underlying medical or surgical problems. On the other hand, chronic abdominal pain, most currently functional in origin, frequently generates a situation of familial and patient stress due to the persistent recurrence of symptoms. The paediatrician can also be affected by this stress and can be ‘forced’ to prescribe multiple unnecessary medical investigations (5.1).
Understanding the neurophysiology of pain perception is crucial to making an appropriate diagnostic approach. Not every pain perceived in the abdomen originates in the abdomen, and not every pain originating in the abdomen is perceived in the abdomen. Furthermore, characteristics of abdominal pain are very diverse; the specific pattern of abdominal pain sensation will help to establish the diagnosis.
5.1 Aetiology of acute and chronic abdominal pain.
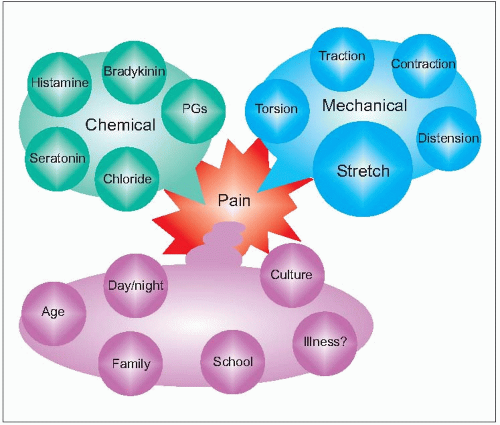
Specific types of pain receptors are located in the abdominal wall, in the mesentery, in the serosal surfaces, in the hollow viscera wall, and in the mucosal surfaces. Main receptors in each location will respond to specific stimuli types. Abdominal pain receptors can be triggered by mechanical and chemical stimuli (5.2). Mechanical stretch and chemical stimuli are the main triggers involved in visceral nociceptor activation.
5.2 Genesis and perception of abdominal pain.
Pain of bilaterally innervated organs (i.e. small intestine) is perceived in the midline. Pain perceived on one side usually comes from nondigestive intra-abdominal organs (ovary, ureters, and kidneys), gallbladder, ascending and descending colon, or abdominal wall which are mainly ipsilaterally innervated.
Chronic abdominal pain
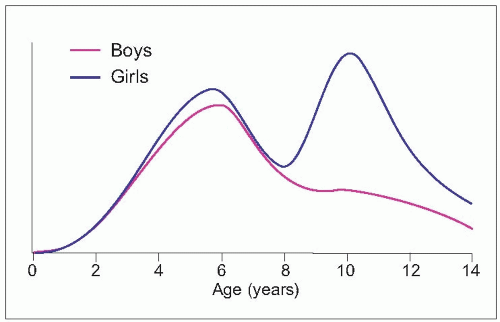
Complaints of recurrent abdominal pain affect 10-40% of children and its prevalence increases with age (5.3)1.
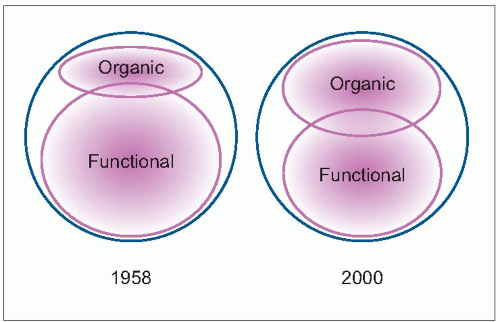
When recurrent abdominal pain was first described in 19582, only 10% of patients had a definitive diagnosis; 90% of patients remained undiagnosed or labelled as ‘suspected functional abdominal pain’. New pathological entities such as Helicobacter pylori infection or non-IgE mediated food allergies and the development of diagnostic techniques has allowed diagnosis to improve to up to 50% of patients (5.4).
In order to avoid unnecessary tests a conservative approach is appropriate. Alarm symptoms, signs, and features that should make the physician suspect that the pain has an organic background are listed in Table 5.1. In their absence, pain is very likely to have a functional origin and therefore most tests will be unnecessary, leading only to increase familial anxiety.
5.3 Incidence of recurrent abdominal pain by age.
5.4 Aetiology of recurrent abdominal pain.
Table 5.1 Alarm symptoms, signs, and features in recurrent abdominal pain
Pain distant from umbilicus (right upper or right lower quadrant pain)
Dysphagia
Persistent vomiting
Gastrointestinal blood loss
Nocturnal and/or severe diarrhoea
Hepatomegaly, splenomegaly
Abdominal mass effect Family history of inflammatory bowel disease, coeliac disease, or peptic ulcer disease
Arthritis
Perirectal disease
Involuntary weight loss
Deceleration of linear growth
Delayed puberty
Dysuria or haematuria
Respiratory symptoms
Tenderness over the spine or at the costovertebral angle
Unexplained fever
Pain that wakes up the child
Functional gastrointestinal disorders
Functional gastrointestinal disorders (FGID) are defined as a variable combination of chronic or recurrent gastrointestinal symptoms not explained by structural or biochemical abnormalities. A symptoms-based classification, rather than a targeted organ-based one, has been set by the Rome III committee (Table 5.2) (5.5)3.
Functional dyspepsia
Dyspepsia is pain or discomfort localized in the upper abdomen. Symptoms may vary including fullness, early satiety, bloating, nausea, retching, and vomiting. No signs or symptoms reliably differentiate functional dyspepsia from upper gastrointestinal organic disorders (Table 5.3)4.
5.5 Overview of abdominal pain-related functional gastrointestinal disease.
To establish the diagnosis of functional dyspepsia (Table 5.4) it is therefore necessary to rule out organic diseases presenting with dyspepsia, such as gastro-oesophageal reflux disease (5.6, 5.7), Helicobacter pylori infection, eosinophilic oesophagitis, and gastritis.
Although presented as independent categories, only a minority of patients shall be classified in any of the first three specific categories (*), while most will fall within the ‘Functional abdominal pain’ open-box category
No signs or symptoms reliably differentiates organic from functional
Functional abdominal pain
Depending on anamnesis
Irritable bowel syndrome
Not required
If diagnostic criteria fulfilled
Abdominal migraine
Not required
If diagnostic criteria fulfilled
Table 5.4 Diagnostic criteria for functional dyspepsia
•
Persistent or recurrent pain or discomfort centred in the upper abdomen (above the umbilicus)
•
Pain not relieved by defecation or associated with onset of a change in stool frequency or consistency
•
No evidence of inflammatory, anatomic, metabolic, or neoplastic process that explains subject’s symptoms
All three criteria must be fulfilled at least once per week for at least 2 months
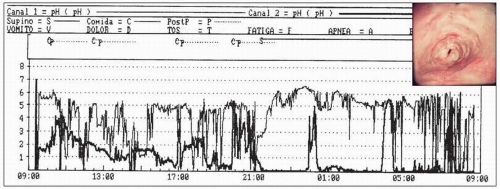
5.6 Gastro-oesophagic reflux. pH study of severe gastro-oesophagic reflux in a 7-year-old patient with epigastric pain, heartburn, and vomiting. Endoscopy of reflux oesophagitis (inset).
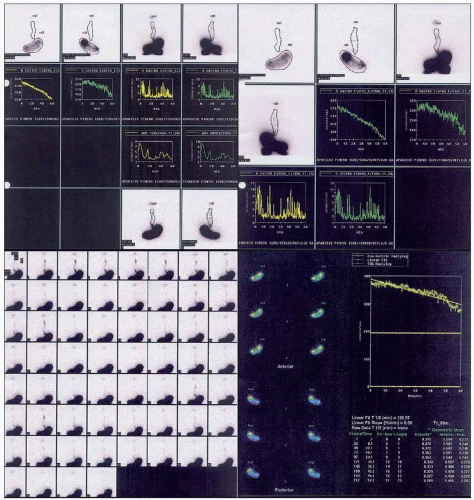
5.7 Gastric emptying scintigraphy. Same patient as in 5.6 after treatment with proton pump inhibitors, showing very slow gastric emptying with associated nonacid gastro-oesophageal reflux.
Irritable bowel syndrome
Irritable bowel syndrome (IBS) is characterized by episodes of recurrent abdominal pain temporally associated with altered bowel habits: either constipation or diarrhoea (Table 5.5). If the child fulfils the diagnostic criteria no further investigations are required. Aetiology of IBS is multifactorial and not completely understood (5.8)5,6. Available therapeutic options are summarized in Table 5.6, although most of these patients’ symptoms improve if they manage to reduce or dominate the stress intervening factors.
Only gold members can continue reading. Log In or Register to continue