Constipation can be defined as the delay or difficulty in defecation occurring for ≥2 weeks and causing significant distress to the patient. As a symptom, constipation can be caused by many different disorders (Table 4.1) but 90% of all constipated children have functional constipation, with no identifiable organic or anatomical cause. Constipation is a common symptom in paediatric clinical practice, accounting for 3% of all general paediatric visits and between 10 and 25% of all cases in paediatric gastroenterology reference units.
Table 4.1 Differential diagnosis of constipation
Functional constipation (90%)
Organic constipation (10%)
•
Anatomical malformations
–
Anal stenosis
–
Imperforatus anus
–
Anterior displaced anus
–
Pelvic mass (sacral teratoma)
•
Neuromuscular disorders
–
Cerebral palsy, hypotonia
–
Disorders of the spinal cord
–
Myelomeningocoele
–
Spinal cord trauma
–
Spinal cord tumour
–
Muscular dystrophy
•
Metabolic and endocrine disorders
–
Hypothyroidism
–
Renal acidosis
–
Diabetes insipidus
–
Hypercalcaemia
–
Hypokalaemia
•
Intestinal nerve or muscle disorders
–
Hirschsprung’s disease
–
Neuronal intestinal dysplasia
–
Chronic intestinal pseudoobstruction
•
Gastrointestinal diseases
–
Coeliac disease
–
Cystic fibrosis
–
Cow’s milk intolerance
•
Abnormal abdominal musculature
–
Prune belly syndrome
–
Gastroschisis
–
Down syndrome
•
Drugs
–
Antacids
–
Codein
–
Phenytoin
–
Opiates
–
Antidepressants
–
Anticholinergics
–
Iron
Normal defecation and functional constipation
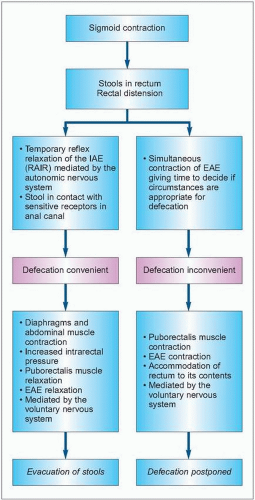
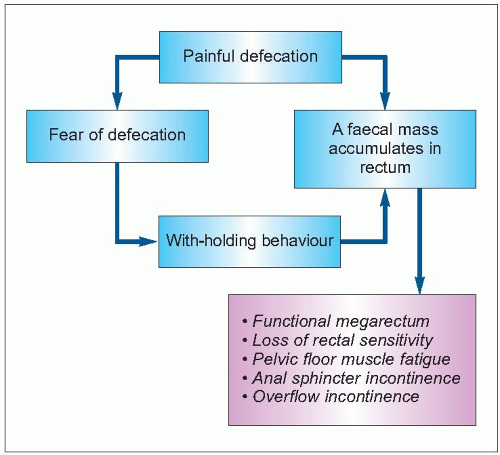
Mechanisms of normal defecation and continence are summarized in figure 4.1. The term ‘functional constipation’ (also called idiopathic or retentive constipation or psychogenic megacolon) describes all children in whom constipation does not have an organic aetiology, and it is generally caused by a maladaptative response to defecation (4.2). In functional constipation, fear of defecation after a painful experience and repeated attempts of voluntary withholding of stools (vicious circle theory) lead to the formation of a functional megarectum with loss of rectal sensitivity and of the normal need to defecate. Progressive accumulation of feces in the rectum leads to pelvic floor muscle fatigue and anal sphincter poor competence, causing overflow incontinence and nonvoluntary expulsion of faeces, or encopresis. Encopresis is the involuntary loss of stool into the child’s underwear in a child with functional constipation after the acquisition of the toilet skills that are acquired by most children by the age of 4 years. Constitutional and inherited factors such as slow intrinsic motility and low fibre diet may contribute to constipation.
4.1 Normal mechanism of defecation and continence. In newborn babies and very young infants, the role played by the cerebral cortex in these events is not yet developed; therefore, defecation occurs when the internal sphincter relaxes. IAE: internal anal sphincter; EAE: external anal sphincter; RAIR: rectoanal inhibitory reflex.
4.2 Pathophysiology of functional constipation.
Onset of functional constipation occurs in one of three periods: (1) in infants, often corresponding with the change from breast milk to commercial formula or introduction of solids, (2) in toddlers acquiring toilet skills, and (3) in children as school starts. Table 4.2 summarizes the main clinical symptoms and complications in children with functional constipation1. Diagnostic criteria for childhood functional gastrointestinal disorders, known as the Rome III criteria have been recently reviewed2,3. Functional disorders of defecation include infant dyschezia and functional constipation in infants and children (Table 4.3).
Table 4.2 Clinical symptoms and complications in children with functional constipation
•
Retentive posturing: affected children are often described as standing on their toes, holding onto furniture, stiffening their legs and hiding in a corner
•
Infrequent and painful passage of huge stools
•
Abdominal pain and irritability, anal or rectal pain
•
Anorexia
•
Encopresis: sometimes is the first symptom and it is confused with chronic diarrhoea
•
Urinary symptoms:
–
Night-time urinary incontinence
–
Daytime urinary incontinence
–
Urinary tract infection
–
Less frequently: vesicoureteral reflux, urinary retention, megacystis, ureteral obstruction
•
Immediate resolution of symptoms after the passage of a huge stool
Must include both of the following in an infant younger than 6 months of age:
1
At least 10 minutes of straining and crying before successful passage of soft stools
2
No other health problems
G7. Functional constipation (neonate and toddler)
Must include 1 month of at least 2 of the following in infants up to 4 years of age
1
Two or fewer defecations per week
2
At least 1 episode per week of incontinence after the acquisition of toileting skills
3
History of excessive stool retention
4
History of painful or hard bowel movements
5
Presence of a large faecal mass in the rectum
6
History of large-diameter stools that may obstruct the toilet
Accompanying symptoms may include irritability, decreased appetite and/or early satiety. The accompanying symptoms disappear immediately following passage of a large stool
H3a. Functional constipation (child and adolescent) Must include 2 or more of the following in a child with a developmental age of at least 4 years*:
1
Two or fewer defecations in the toilet per week
2
At least 1 episode per week of incontinence
3
History of retentive posturing or excessive volitional stooling retention
4
History of painful or hard bowel movements
5
Presence of a large faecal mass in the rectum
6
History of large diameter stools that may obstruct the toilet
* Criteria fulfilled at least once per week for at least 2 months before diagnosis
Infant dyschezia
Some otherwise healthy infants less than 6 months of age appear to have significant discomfort and excessive straining associated with passing soft stools. The symptoms resolve spontaneously after a few weeks and are probably related to a failure to coordinate increased intra-abdominal pressure with pelvic floor relaxation. Parents need to be reassured that the phenomenon is part of the child’s learning process and that no intervention is necessary. Rectal stimulation should be avoided to prevent artificial sensory experiences and laxatives are unnecessary.
Functional constipation
The definition of functional constipation takes into account not only the frequency of stools but also the passage of painful bowel movements and stool retention with or without encopresis. Normal stool frequency ranges from four per day during the first week of life to two per day at 1 year of age. The normal adult range of three per day to three per week is attained by 4 years of age. Some breastfed babies have very infrequent stools of normal consistency without distress; these infants are usually perfectly healthy and infrequent stools relate to almost complete absorption of breast milk, leaving very little residue for stool formation.
Hirschsprung’s disease
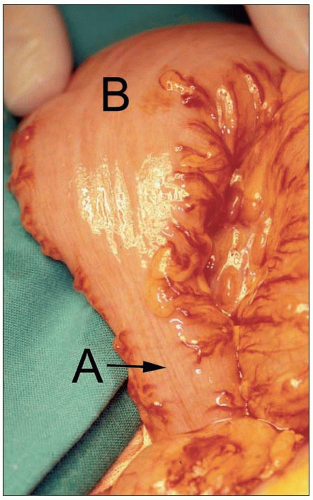
Hirschsprung’s disease, with an incidence of 1 in 5,000 live births, is the most frequent cause of lower intestinal obstruction in newborns. It is found in about 3% of children and toddlers with severe refractory constipation referred to the paediatric gastroenterologist (4.3). Hirschsprung’s disease is characterized by the absence of ganglion cells in the myenteric and submucosal plexuses of the colon leading to sustained contraction of the aganglionic segment. The bowel proximal to the aganglionic segment becomes dilated with secondary intestinal ischaemia that contributes to enterocolitis. The aganglionic segment begins in the internal anal sphincter and extends proximally, in 75% of cases to the rectosigmoid area, in 20% to the colon proximal to the splenic flexure, in 3-5% there is total colonic aganglionosis and, even less frequently, there is total intestinal aganglionosis. There is also a very rare form of the disease in which there is an ultra-short segment involving only the very distal 2-5 cm of the rectum.
4.3 Hirschsprung’s disease is characterized by the absence of ganglion cells in the myenteric and submucosal plexuses of the colon leading to sustained contraction of the aganglionic segment (A). The bowel proximal to the aganglionic segment becomes dilated (B) with secondary intestinal ischaemia that contributes to enterocolitis.
Symptoms and signs of Hirschsprung’s disease are summarized in Table 4.4. Enterocolitis is the most serious complication and it could be the first manifestation of the disease. It is characterized by the abrupt onset of fever, abdominal distention, and explosive and sometimes bloody diarrhoea, mainly in 2-3-month-old infants and is associated with a mortality of 20%. Mortality is reduced with early diagnosis of Hirschsprung’s disease.
Table 4.4 Signs and symptoms suggestive of Hirschsprung’s disease (HD) in constipated children
Symptoms
•
Constipation beginning early in life
•
Delayed passage of meconium
•
Failure to thrive
•
Abdominal distention
•
Absence of encopresis
•
Fever, bloody diarrhoea (enterocolitis)
•
Chronic constipation not responding to treatment
Signs
•
Passage of liquid stools and gas after rectal digital examination
•
Empty rectal vault (although stool is palpable in the abdomen)
•
Increased anal tone
•
Signs of syndromes associated with HD
–
Down syndrome
–
Multiple endocrine neoplasia IIA
–
Congenital deafness
–
Waardenberg’s syndrome
–
Neurofibromatosis
Only gold members can continue reading. Log In or Register to continue