Fig. 17.1
Express procedure for intussusception. a A purpose-designed tunneller is inserted via the perineal wound (lateral to the vagina) upwards behind the pubic bone to emerge through the suprapubic wound taking great care to prevent injury to the bladder. b The sharp point of the tunneller is replaced by a plastic olive, which has attached to it a T-shaped strip of Permacol™. c The Permacol™ strip is drawn down to the perineal wound and positioned so the transverse part of the strip lies on the anterolateral wall of the rectum at approximately 8 cm above the superior border of the sphincter complex. The second strip is similarly placed on the opposite side. d After gentle upward traction on the Permacol™ strips, they are sutured to the periosteum of the pubic bone. (Reproduced from [1], with permission)
The sharp point of the tunneller is replaced by a plastic olive which has attached to it a T-shaped strip of Permacol™ (Fig. 17.1b). This strip is then drawn down to the perineal wound and its transverse part, measuring 2 cm in width, is sutured to the anterolateral rectal wall with two 0 PDS™ sutures with its lower edge at approximately 6–8 cm above the superior border of the sphincter complex (Fig. 17.1c). The vertical part of the strip is left emerging from the suprapubic wound with an artery forceps attached. This maneuver is repeated on the opposite side. Once in place, vertical traction is exerted on the strips via the suprapubic wounds. Once firm but not excessive traction of the rectal wall is achieved, the proximal parts of the T-shaped strips of Permacol™ are sutured to the periosteum of the pubic bone with the two interrupted 0 PDS™ sutures previously placed (Fig. 17.1d). If a rectocele is also present, it can be repaired at the same time using a patch of Permacol™. The patch is shaped 5 ± 5 cm in size with two extensions on the lateral sides. The patch is sutured over the anterior rectal wall with interrupted 2.0 PDS™ sutures (Fig. 17.2). The lateral wings are routed behind the puborectalis and sutured to the periosteum overlying the medial aspect of the ischium in line with the rectocele on either side with two sutures of 0 PDS™ on a J needle. This is performed from within the perineal wound, the rationale being to reinforce the rectovagianal septum and at the same time limit the anterior protrusion and ballooning effect of the anterior rectal wall causing the rectocele.
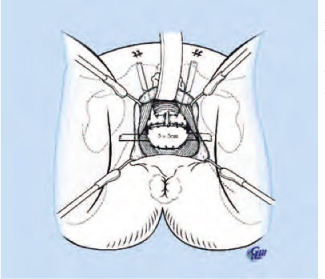
Fig. 17.2
Concomitant rectocele repair. A patch of Permacol™ is sutured over the defect in the rectovaginal septum and the wings are sutured to the ischial tuberosities. (Reproduced from [1], with permission)
17.4 Results
Our initial experience with this procedure included 17 patients [1]. Thirteen patients (all female) had a concomitant rectocoele repair. Clinical details are summarized in Table 17.1. The median follow-up period was 12 months (range 6–20 months).
Table 17.1
Demographics and symptoms for patients with rectal intussusception (n = 17)
Patient characteristics and symptoms | |
Age (years) | 47 (20–67) |
Gender (M:F) | 4:13 |
Symptom duration (months) | 36 (5–400) |
Previous pelvic surgery (n) | 9 (2 gracilis neosphincter, 4 colposuspension, 3 hysterectomy) |
Parity | 3 (0–5)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|



