MDACC
AHPBA/SSO/SSAT
NCCN
Celiac axis (CA)
No extension
Clear fat plane around CA
No contact
Common hepatic artery (CHA)
No extension
Clear fat plane around CHA
No contact
Superior mesenteric artery (SMA)
No extension; normal fat plane between tumor and SMA
Clear fat plane around SMA
No contact
Superior mesenteric vein-portal vein (SMV–PV) confluence
Abutment or encasement with patent vessels (no occlusion)
No abutment, distortion, tumor thrombus, or encasement
No contact OR ≤180° contact without vein contour irregularity
Definitions of Resectable Disease
Uniformly, resectable disease includes tumors that do not appear to contact the CA, HA, SMA, or SMV given that a margin-negative resection can often be achieved without any prior therapy in patients with these tumors. More recently, several groups have also considered as resectable tumors with limited involvement of the SMV–PV confluence in which an R0 resection is still possible, albeit with vascular resection and reconstruction. For example, the definition used at MDACC considers tumors resectable if there is abutment of the SMV–PV with patent vessels (no occlusion) [20]. The NCCN definition also classifies as resectable any tumor with ≤180° contact of the SMV–PV but without any vein contour irregularity [21] (Table 1.1, Fig. 1.1).
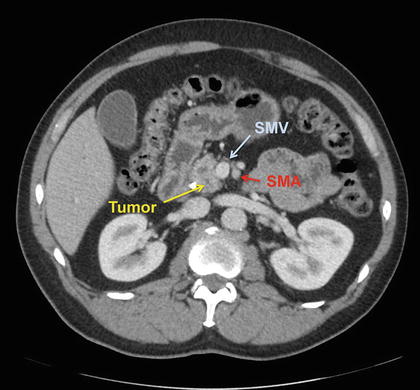
Fig. 1.1
CT scan demonstrating resectable pancreatic adenocarcinoma of the head with SMV abutment of less than 180° and a clear fat plane between the tumor and the SMA
Definitions of Locally Advanced Disease
Definitions of locally advanced disease (LAD) also vary, although in general, LAD characterizes those patients in whom the likelihood of response to non-operative therapy sufficient to allow for a subsequent margin-negative resection is nearly zero. For example, according to the MDACC definition, locally advanced disease consists of tumors that involve the SMA greater than 180°, those that encase the CA or CHA without a technical option for reconstruction, and those which occlude the SMV–PV with no technical option for reconstruction [20].
The NCCN considers tumors of the pancreatic head and uncinate process locally advanced if the tumor demonstrates contact with the first jejunal vein draining into the SMV or an unreconstructable SMV–PV confluence. Tumors with >180° contact with the SMA, CA, or contact the first jejunal arterial SMA branch are also considered locally advanced. Body and tail tumors are considered locally advanced if the SMV–PV confluence is involved and unreconstructable or if there is contact of >180° with the SMA or HA, or with the CA and aorta (Table 1.2, Figs. 1.2 and 1.3).
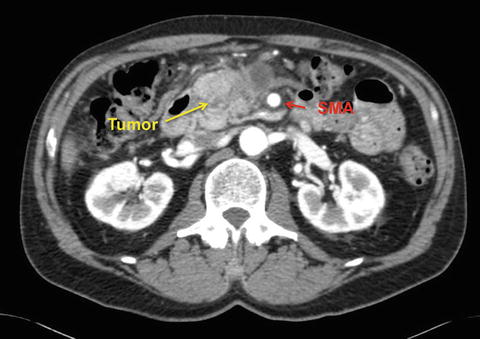
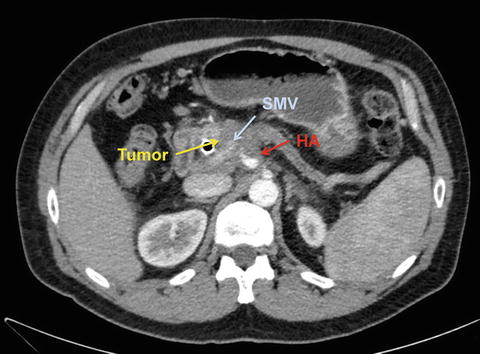
Table 1.2
Locally advanced (unresectable) pancreatic cancer definitions
MDACC | AHPBA/SSO/SSAT | NCCN | |
|---|---|---|---|
Celiac axis (CA) | Encasement | Abutment or encasement | Contact >180° |
Common hepatic artery (CHA) | Encasement with no technical option for reconstruction | Encasement with extension to celiac axis | Contact with extension to CA or bifurcation |
Superior mesenteric artery (SMA) | Encasement >180° | Encasement >180° | Contact >180° or contact with first jejunal SMA branch |
Superior mesenteric vein-portal vein (SMV–PV) confluence | Occluded and no technical option for reconstruction | Occlusion without options for reconstruction | Unreconstructible due to tumor involvement or occlusion, contact with proximal jejunal branch |
Fig. 1.2
CT scan of a locally advanced pancreatic adenocarcinoma with obliteration of the SMV at the base of the mesentery, leaving no distal venous target for reconstruction
Fig. 1.3
CT scan of a locally advanced pancreatic adenocarcinoma with encasement of the SMV as well as the CHA (common hepatic artery)
Definitions of Borderline Resectable Disease
The definition of borderline resectable (BRPC) , first termed marginally resectable, was first described in 2001 in a prospective case series by Mehta et al. and was intended to describe patients at high risk of grossly positive margins with immediate resection [22]. Patients were treated with 5-FU and radiation therapy and then re-evaluated for resection; 9 of 15 patients subsequently underwent resection with negative margins [22]. In 2006, the NCCN first adopted the term “borderline resectable” to characterize the group of patients at high risk for a margin-positive resection and for whom administration of neoadjuvant therapy should be considered.
Over the past decade, a number of different radiographic classification schemes have been subsequently developed to describe which patients are considered borderline resectable, including consensus statements and guidelines from not only the NCCN, but also the International Study Group of Pancreatic Surgery (ISGPS); MDACC; Americas Hepato Pancreato-Biliary Association (AHPBA), Society of Surgical Oncology (SSO), and Society for Surgery of the Alimentary Tract (SSAT) [20, 23, 24]. A definition has also been established within the context of a now-completed multi-institutional prospective trial, the Intergroup borderline resectable pilot study (Alliance A021101) [25]. These criteria have been endorsed by the NCCN and are summarized in Table 1.3 and shown with representative CT scans in Figs. 1.4, 1.5, and 1.6. To date, no single definition has been used uniformly.
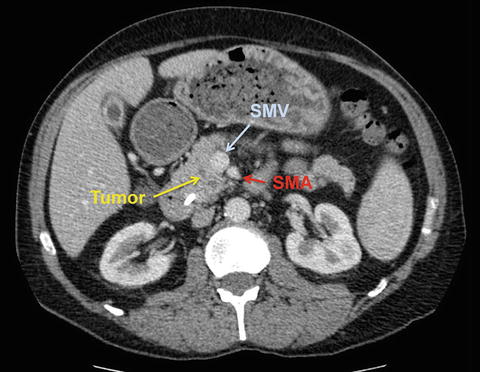
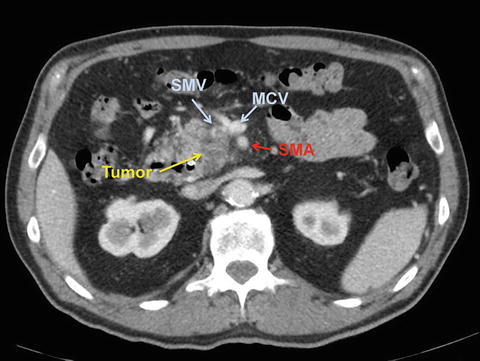
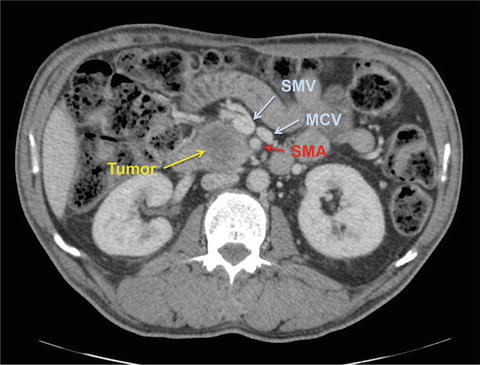
Table 1.3
Borderline resectable pancreatic cancer definitions
MDACC | AHPBA/SSO/SSAT | NCCN/ISGPS | Moffitt | Intergroup (Alliance A021101) | |
|---|---|---|---|---|---|
Celiac axis (CA) | Abutment | No abutment or encasement | Contact ≤180° or contact >180° with uninvolved GDA | Not specified | Interface between tumor and vessel <180° circumference vessel wall |
Common hepatic artery (CHA) | Abutment or short segment encasement | Short segment abutment or encasement amenable to reconstruction | GDA encasement to hepatic artery with short segment encasement or direct abutment without extension to hepatic bifurcation or celiac axis | Encasement of GDA up to origin of CHA | Reconstructible, short-segment interface between tumor and vessel of any degree |
Superior mesenteric artery (SMA) | Abutment <180° | Abutment <180° | Contact ≤180° | Circumferential tumor abutment <180° | Interface between tumor and vessel measuring <180° circumference of vessel wall |
Superior mesenteric vein-portal vein (SMV–PV) confluence | Short segment occlusion amenable to resection and reconstruction | Abutment >180° or occlusion amenable to resection and reconstruction | Contact of >180°, contact of ≤180° with irregularity of vein or thrombosis amenable to resection and reconstruction | Circumferential abutment or encasement amenable to resection and reconstruction | Interface between tumor and vessel measuring 180° or greater of circumference of vessel wall, and/or reconstructable occlusion |
Fig. 1.4
CT scan demonstrating a borderline resectable pancreatic adenocarcinoma with SMV abutment of approximately 180° and subtle haziness posterior to the SMA
Fig. 1.5
CT scan demonstrating a borderline resectable pancreatic adenocarcinoma with tumor thrombus within the SMV
Fig. 1.6
CT scan demonstrating a borderline resectable pancreatic adenocarcinoma with SMV abutment of approximately 180° at the base of the mesentery and haziness around the SMA
The most recent NCCN guidelines outline a definition of BRPC as tumor demonstrating radiographic contact with the SMV–PV of >180°, or contact of ≤180° with contour irregularity or thrombosis of the vein but with suitable vessel proximal and distal to the site of involvement to allow for adequate resection [21]. Solid tumor contact with the IVC is also considered borderline resectable. Regarding arterial involvement, NCCN considers tumor contact with CHA without extension to CA or HA bifurcation and ≤180° contact with SMA to be borderline resectable for pancreatic head lesions. A tumor within the body or tail is considered borderline resectable if there is contact ≤180° with CA or >180° of CA without involvement of aorta and with an uninvolved, intact GDA.
The MDACC definition published in 2006 allows for short segment occlusion of the SMV–PV as long as a suitable vessel is available above and below the involved segment for reconstruction [20]. Additionally, tumor abutment of ≤180° of the circumference of the SMA and short segment encasement or abutment of the CHA (usually at the GDA origin) is considered potentially resectable. In follow-up work, Katz et al. elaborated on these definitions further, to not only account for anatomical feasibility but also clinical appropriateness for pancreatectomy [26]. MDACC categorized patients into three subsets: Group A comprised patients meeting the anatomic criteria listed above; Group B consisted of patients with preoperative work-up suggestive but not diagnostic of metastasis; and Group C was made up of patients with comorbidities or those with a marginal, but potentially reversible, performance status (typically ECOG 2-3). Group B patients had CT findings suspicious for but not diagnostic of metastatic disease (indeterminate subcentimeter liver lesions or peritoneal or omental nodules too small for biopsy) or known N1 disease as determined by EUS-FNA or pre-referral laparotomy.
Related posts:
 Overview of Multimodality Therapy
Emerging Systemic and Targeted Therapies
Overview of Multimodality Therapy
Emerging Systemic and Targeted Therapies
 Palliative Operations for Unresectable Pancreatic Cancer
Palliative Operations for Unresectable Pancreatic Cancer
 Role of Radiation Therapy
Role of Radiation Therapy
 Endoscopic and Percutaneous Biliary Drainage Procedures: Role in Preoperative Management, Diagnosis, and Palliation
Endoscopic and Percutaneous Biliary Drainage Procedures: Role in Preoperative Management, Diagnosis, and Palliation
 Endoscopic Ultrasonography: Staging and Therapeutic Interventions
Endoscopic Ultrasonography: Staging and Therapeutic Interventions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


