Which Renal Cysts Require Follow-up Evaluation?
With the ubiquitous imaging being performed today, it is very common to discover incidental renal cysts. Clinicians usually turn to nephrologists to ask what to do about them.
CLINICAL AND RADIOLOGIC CHARACTERISTICS
Most renal cysts in adults are simple renal cysts. A cyst is a sac of clear, serous fluid (ultrafiltrate of plasma) that is lined by a single layer of epithelial cells. Renal cysts are derived from progressive dilatation and detachment of diverticula in the distal convoluted tubule and collecting duct. Incidental cysts may be solitary or multiple, and their frequency increases with age. (Up to 50% of patients aged 40-50 years will have cysts.) Patients are usually asymptomatic but rarely may have abdominal or flank discomfort or develop hematuria or symptoms and signs of infection. Hypertension due to cyst compression of normal renal tissue is rare. Diagnosis is generally made as an incidental finding on renal or abdominal ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI).
On renal ultrasound, simple cysts are typically round and sharply demarcated with smooth walls and without echoes within the cyst (Fig. 17.1). Sometimes there may be thin internal septations (Fig 17.2). A strong posterior wall echo indicating good transmission through the cyst and enhanced transmission beyond the cyst are characteristic. Such cysts are benign and do not require follow-up imaging. The primary clinical concern is accurately distinguishing simple renal cysts from complex renal cysts, the latter of which are associated with an increased risk of malignancy and do require follow-up and/or further testing. Some cysts
cannot be characterized noninvasively with certainty, and may require biopsy or surgical excision for diagnosis.
cannot be characterized noninvasively with certainty, and may require biopsy or surgical excision for diagnosis.
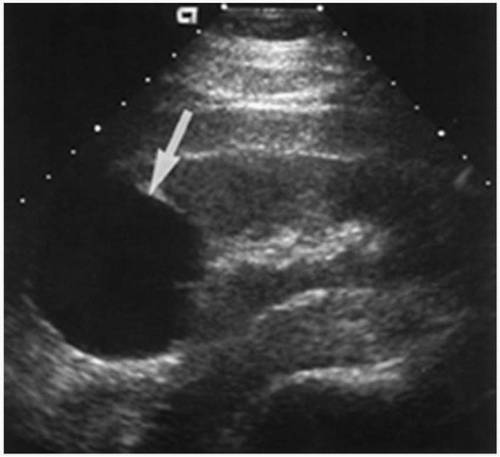 FIGURE 17.1 Simple cyst on renal ultrasound. |
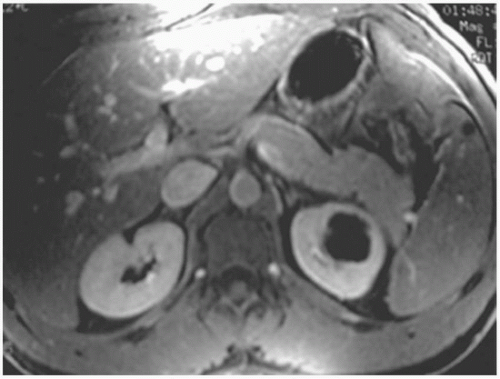 FIGURE 17.2 Septated renal cyst on renal ultrasound. |
Occasionally, autosomal dominant polycystic kidney disease (PKD) will be discovered on renal imaging; in this disorder, the kidneys will be large (sometimes very large) and filled with innumerable renal cysts. There will generally be a family history of the disorder as well as coexisting
liver cysts. Acquired cystic disease, characterized by multiple renal cysts in patients with end-stage renal disease (ESRD), usually after several years of dialysis, can also be easily detected; in this case, the noncystic renal tissue is atrophic. Smaller cysts, usually less than 1 cm in diameter, occur in medullary sponge kidney, autosomal recessive PKD, and autosomal dominant interstitial kidney disease (previously called medullary cystic kidney disease).
liver cysts. Acquired cystic disease, characterized by multiple renal cysts in patients with end-stage renal disease (ESRD), usually after several years of dialysis, can also be easily detected; in this case, the noncystic renal tissue is atrophic. Smaller cysts, usually less than 1 cm in diameter, occur in medullary sponge kidney, autosomal recessive PKD, and autosomal dominant interstitial kidney disease (previously called medullary cystic kidney disease).
When ultrasonography is inconclusive, radiologists generally recommend a renal CT with contrast (unless there is renal failure). CT criteria to distinguish benign from complex cysts have been developed. Using the Bosniak classification, cysts can be classified on the basis of morphologic and contrast enhancement characteristics (Israel and Bosniak, 2005):
Category I: Benign simple cyst with a thin wall without septa, calcifications, or solid components; water density; no contrast enhancement; no follow-up needed (Fig. 17.3A).
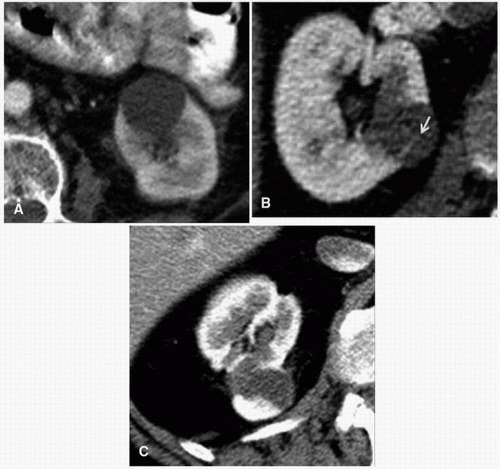 FIGURE 17.3 CT showing a simple category I kidney cyst (A), a simple Category IIF cyst containing thin internal septae (arrow) (B), and cystic adenocarcinoma (Category IV cyst) (C). |
Category II: Benign cystic lesions in which there may be a few thin septa; the wall or septa may contain fine calcification or a short segment of slightly thickened calcification; less than 3 cm in diameter, well-marginated, no measurable contrast enhancement; no follow-up needed (Fig. 17.3B).
Category IIF: Multiple thin septa or minimal smooth thickening of the septa or wall, which may contain calcification that may also be thick and nodular; no measurable contrast enhancement; may be more than 3 cm in diameter; require follow-up to ascertain that they are nonmalignant.
Category III: Indeterminate cystic masses with thickened irregular or smooth walls or septa; measurable contrast enhancement is present; risk of malignancy is about 50% (cystic renal cell carcinoma and multiloculated cystic renal cell carcinoma); require further imaging and consideration of surgery.
Related posts:
 What Is Fractional Excretion and How Does Measuring It Help in Clinical Practice?
What Is Fractional Excretion and How Does Measuring It Help in Clinical Practice?
 How Is the Urinalysis Helpful in Patients with Kidney Disease?
What Is Free Water Clearance and How Useful Is It?
How Does One Interpret the Urine Anion Gap and Urine Osmolal Gap?
How Is the Urinalysis Helpful in Patients with Kidney Disease?
What Is Free Water Clearance and How Useful Is It?
How Does One Interpret the Urine Anion Gap and Urine Osmolal Gap?
 Is There a Risk to Rapidly Lowering the Plasma Potassium in Patients with Hyperkalemia?
Should Calcium-Based Phosphate Binders Be Used in Patients with Chronic Kidney Disease?
Is There a Risk to Rapidly Lowering the Plasma Potassium in Patients with Hyperkalemia?
Should Calcium-Based Phosphate Binders Be Used in Patients with Chronic Kidney Disease?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


