CHAPTER 6 WEDGE RESECTION AND ENUCLEATION TECHNIQUES: HEPATIC ARTERY INFUSION CHEMOTHERAPY
WEDGE RESECTION
Wedge resection of peripherally placed lesions within the liver is carried out easily for tumors measuring up to 2 to 3 cm in diameter. However, lesions occupying the convex surface of the liver and away from the free edge, such as lesions within segment VIII, are much more difficult to approach. Wedge resections, especially for lesions situated on the dome of the liver, are fraught with difficulty, not only regarding the control of hemorrhage within the depths of the wedge, but also in obtaining tumor-free margins. Because of this, wedge resections of the liver have been shown to be associated with a high local recurrence rate (DeMatteo et al., 2000). One of the reasons for this is the likelihood of fracturing the specimen along the interface of the hard tumor and the surrounding soft liver. Certainly for tumors lying well within the substance of the liver and for larger tumors, an anatomic resection, as described in Chapters 2 through 5, is the preferred approach.
CRYO-ASSISTED HEPATIC RESECTION
Cryoablation is a recognized approach to the treatment of malignant tumors. The use of the cryoprobe as a device to assist during wedge resection also has been developed (Polk et al., 1995). Cryo-assisted resection may be used in three particular instances:
Technique
Glisson’s capsule is scored with a diathermy at the point of insertion of the selected cryoprobe (Fig. 6-1). The probe is inserted under direct vision and guided by ultrasound to the center of the lesion. Laparotomy pads are placed to protect adjacent structures. Pringle’s maneuver (Pringle, 1908) is applied before start of the freeze cycle. The freeze cycle is initiated, and ultrasound is used to monitor freezing. The freeze margin is easily seen as a hyperechoic rim with posterior acoustic shadowing slowly developing from the center of the lesion. The freeze margin is allowed to reach a distance of approximately 1 cm outside the periphery of the tumor (see Fig. 6-1). At this point, hepatic vascular inflow occlusion is temporarily released. Two minutes are allowed for reperfusion of the liver, and then the Pringle maneuver is reinstituted during resection of the parenchyma. To maintain the ice ball at a constant size during resection, freeze and thaw cycles of 1 minute each during the resection procedure are allowed. This cycling is successful in preventing extension of the ice ball or inadvertent removal of the probe, which can be used as a “handle” to manipulate the lesion during resection. Dissection is performed directly on the ice ball or at a slight distance from it (see Fig. 6-1). Traction on the cryoprobe and ice ball complex provides exposure during the parenchymal transection. Blood vessels are easily visualized and are individually controlled as they are encountered. In patients in whom the tumor is shown on ultrasound to approximate a major venous structure (e.g., the right hepatic vein), preliminary mobilization of the liver from the underlying vena cava, isolation of the right hepatic vein, and temporary clamping of the vein during the procedure have allowed safe resection.
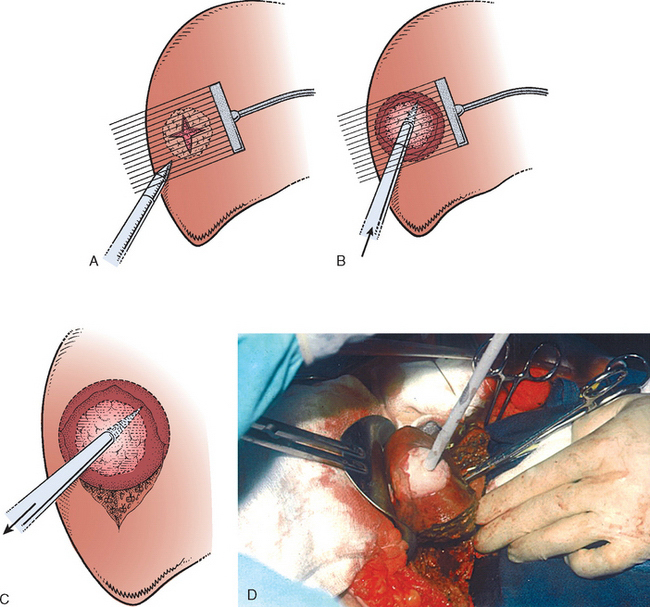
The specimen is left attached to the cryoprobe (see Fig. 6-1






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


