Vomiting is a complex behaviour composed of three linked activities: nausea, retching, and expulsion of stomach contents. The vomiting act is characterized by cycles of retching followed by forceful expulsion of gastric contents through the mouth. Although it was previously thought one or two anatomical vomiting centres existed in the central nervous system (CNS), it is now assumed that the central vomiting centres represent the integrated activity of the paraventricular nuclei arrayed along the central neuraxis controlling a myriad of autonomic functions1.
Vomiting may result from a variety of disorders affecting paediatric patients (Table 2.1). History and physical examination may help us to distinguish nonbilious from bilious causes, i.e. proximal or distal to the ampulla of Vater.
Evaluation
Vomiting is a common symptom of many disease states. The differential diagnosis of the child with vomiting varies with the age of the patient. Assessment of the child with vomiting should start with a complete history, physical examination, and description of the vomitus. Emesis of gastric contents is characteristic of gastric outlet obstruction, CNS masses or infection, peptic disease, urinary tract infection, otitis, inborn error of metabolism, or psychogenic vomiting. The child who vomits bile-stained material may have an intestinal obstruction and should be investigated urgently. The history and physical examination are essential starting points and should include duration of vomiting, presence of blood, abdominal pain, or fever. Pain located in the right lower quadrant suggests appendicitis. Midline or diffuse abdominal pain suggests pancreatitis or peritonitis. Abdominal distension suggests intestinal obstruction. Viral or bacterial gastroenteritis are usually accompanied by diarrhoea and fever. The presence of mucus and blood in the stool may raise the suspicion of intussusception or bacterial or toxic colitis. The evaluation of bloody vomitus start with the confirmation that the material vomited is blood.
Imaging may help to rule out anatomical causes or intestinal obstruction. Further evaluation may include blood count, serum electrolytes, calcium, magnesium, blood urea nitrogen, urinalysis, and culture, and stool examination for occult blood, leukocytes, and parasites. Specific indications from history and physical examination may result in obtaining other tests including abdominal ultrasonography, imaging of the head, test of liver function, serum amylase, toxicology screen, serum ammonia, urinary organic acids, and so on. If there is a bloody vomitus, the most productive test is upper intestinal endoscopy.
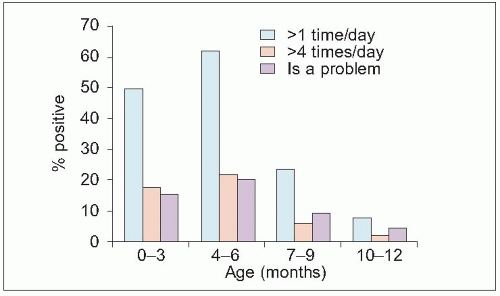
2.1 Reported regurgitation according to age.
Gastro-oesophageal reflux and regurgitation
This is defined as effortless expulsion of gastric contents by the mouth and can be asymptomatic or symptomatic. Gastro-oesophageal reflux disease (GERD) is defined as gastro-oesophageal reflux (GER) that occurs too frequently and damages the oesophageal mucosa leading to clinical symptoms. Spontaneous relaxation of the lower oesophageal sphincter is the major mechanism by which GER occurs, with or without regurgitation2. GER is a physiological event that can be seen in a large number of infants: >50% of 2-month-old infants regurgitate twice a day. The highest prevalence is at 4 months, when two-thirds of infants regurgitate. By 1 year, <10% still present vomiting daily. GERD affects a much smaller proportion of infants (2.1).
Symptoms/examination
The most common symptom is postprandial regurgitation of effortless spit-up. Severe GERD may present with failure to thrive, oesophagitis with haematemesis, dysphagia, heartburn or chest pain, anaemia, aspiration, chronic cough, and wheezing. Rumination is sometimes a symptom as well as neck contortions (Sandifer’s syndrome). Apnoeic episodes in neonates and very young infants can be caused by reflux. GERD is common in neurologically impaired children.
If not treated, GERD can lead to Barrett’s oesophagus. This is a metaplasia of the oesophageal squamous epithelium that transforms to specialized columnar epithelium; it is a premalignant condition associated with dysplasia and adenocarcinoma. Peptic strictures can present in cases of severe but asymptomatic oesophagitis.
Only gold members can continue reading. Log In or Register to continue