Women are making great strides at all levels of medicine, including gastroenterology. The proportion of women members in gastroenterology societies has increased nearly 2-fold and the percent of women trainees is 36%. Although there continue to be challenges for women in academic and community practice, the American Gastroenterological Association, American Society of Gastrointestinal Endoscopy, and other gastroenterology societies have dedicated substantial resources to foster careers of women in gastroenterology and develop women as leaders in our societies. This article outlines ongoing challenges for women in gastroenterology and some key initiatives addressing barriers to success.
Key points
- •
An increasing percentage of gastroenterologists in the United States are women and they are in demand in both academic and community practices.
- •
Requests for women gastroenterologists by patients continues to increase.
- •
Specific initiatives by the American Gastroenterological Association, American Society of Gastrointestinal Endoscopy foster growth of women’s careers and provide opportunities to work into leadership roles.
Introduction: barriers to entry and the leaky pipeline
Choosing gastroenterology as a career was a natural choice for the 2 authors of this article. Our decisions were driven in part by our belief that, as gastroenterologists, we would impact patient’s lives, be intellectually challenged as we care for people with complex diseases and that we would be able to use exciting and emerging endoscopic tools to alleviate suffering, prevent cancer, and cure disease. We envisioned a satisfying lifestyle that was compatible with family priorities. The 2 authors, however, faced different landscapes and encountered unique challenges based in part on their different genders. Those differences are the subject of this joint publication, written from the viewpoint of 2 immediate past presidents of gastroenterology societies.
Currently, there are approximately 13,000 active US-based gastroenterologists with the vast majority engaged in direct patient care. Although women comprise one-third of active physicians in all specialties, the proportion of women in gastroenterology still is only 15%, ranking among the lowest for specialty choice among women physicians. Reasons for this gender gap are varied and complex. One key factor influencing how women physicians choose a career is the definition of what constitutes a “suitable” lifestyle, which is often defined by senior physicians who are almost all men. Even more complex are factors that lead women physicians to exit from careers at times when men are focused on advancing their careers and are stepping into leadership roles ( Box 1 ).
Structural factors
- •
Lack of networking opportunities that informally create and fertilize catalyst and mentor connections.
- •
Lack of mentors and sponsors.
- •
Amounts and types of support.
- •
Positions in education and training that are less likely to lead to research productivity.
- •
Time constraints of training.
- •
Impact of training on decisions regarding pregnancy and family expansion.
- •
Child care-related responsibilities.
- •
Elder care-related responsibilities.
- •
Other responsibilities regarding household management.
Cultural factors
- •
Gender stereotyping that may inform choice of career focus.
- •
Networking opportunities.
- •
Differences in performance expectations and leadership skills.
- •
Lack of female role models in positions of visibility, influence, and leadership.
- •
Perceived inconsistency with work–life balance.
Individual mindsets
- •
Personal control decisions.
- •
Lack of job satisfaction.
- •
Lack of self-confidence.
- •
Decreased ambition over time.
- •
Uncertain career clarity.
Institutional mindsets
- •
Insidious or subtle biases about subspecialization or procedural training.
- •
Hiring decisions or assignments that intentionally or unintentionally convey bias.
- •
Differences in promotion decisions based on gender.
- •
Differences in publication acceptance, funding, or other objective measures of success, based on gender.
- •
Failure in accountability.
- •
Inflexibility in traditional work hour expectations.
- •
Absence of programs that promote work–life balance.
We all begin our careers with ambition; however, this ambition can fade or be eclipsed by competing priorities. For example, women still provide a disproportionate share of childcare and housework at every career level, even those in the younger generations, among women professionals and in families where both partners work full time. As a result of these and other factors discussed later in this paper, advancement opportunities decline or disappear over a career span more often in women than in men. A major focus of this article discusses how medical societies such as the American Society for Gastrointestinal Endoscopy (ASGE) and the American Gastroenterological Association (AGA) must provide leadership and a proactive approach to understanding and reducing external barriers encountered by women in our specialty.
Introduction: barriers to entry and the leaky pipeline
Choosing gastroenterology as a career was a natural choice for the 2 authors of this article. Our decisions were driven in part by our belief that, as gastroenterologists, we would impact patient’s lives, be intellectually challenged as we care for people with complex diseases and that we would be able to use exciting and emerging endoscopic tools to alleviate suffering, prevent cancer, and cure disease. We envisioned a satisfying lifestyle that was compatible with family priorities. The 2 authors, however, faced different landscapes and encountered unique challenges based in part on their different genders. Those differences are the subject of this joint publication, written from the viewpoint of 2 immediate past presidents of gastroenterology societies.
Currently, there are approximately 13,000 active US-based gastroenterologists with the vast majority engaged in direct patient care. Although women comprise one-third of active physicians in all specialties, the proportion of women in gastroenterology still is only 15%, ranking among the lowest for specialty choice among women physicians. Reasons for this gender gap are varied and complex. One key factor influencing how women physicians choose a career is the definition of what constitutes a “suitable” lifestyle, which is often defined by senior physicians who are almost all men. Even more complex are factors that lead women physicians to exit from careers at times when men are focused on advancing their careers and are stepping into leadership roles ( Box 1 ).
Structural factors
- •
Lack of networking opportunities that informally create and fertilize catalyst and mentor connections.
- •
Lack of mentors and sponsors.
- •
Amounts and types of support.
- •
Positions in education and training that are less likely to lead to research productivity.
- •
Time constraints of training.
- •
Impact of training on decisions regarding pregnancy and family expansion.
- •
Child care-related responsibilities.
- •
Elder care-related responsibilities.
- •
Other responsibilities regarding household management.
Cultural factors
- •
Gender stereotyping that may inform choice of career focus.
- •
Networking opportunities.
- •
Differences in performance expectations and leadership skills.
- •
Lack of female role models in positions of visibility, influence, and leadership.
- •
Perceived inconsistency with work–life balance.
Individual mindsets
- •
Personal control decisions.
- •
Lack of job satisfaction.
- •
Lack of self-confidence.
- •
Decreased ambition over time.
- •
Uncertain career clarity.
Institutional mindsets
- •
Insidious or subtle biases about subspecialization or procedural training.
- •
Hiring decisions or assignments that intentionally or unintentionally convey bias.
- •
Differences in promotion decisions based on gender.
- •
Differences in publication acceptance, funding, or other objective measures of success, based on gender.
- •
Failure in accountability.
- •
Inflexibility in traditional work hour expectations.
- •
Absence of programs that promote work–life balance.
We all begin our careers with ambition; however, this ambition can fade or be eclipsed by competing priorities. For example, women still provide a disproportionate share of childcare and housework at every career level, even those in the younger generations, among women professionals and in families where both partners work full time. As a result of these and other factors discussed later in this paper, advancement opportunities decline or disappear over a career span more often in women than in men. A major focus of this article discusses how medical societies such as the American Society for Gastrointestinal Endoscopy (ASGE) and the American Gastroenterological Association (AGA) must provide leadership and a proactive approach to understanding and reducing external barriers encountered by women in our specialty.
Why women in gastroenterology matter
Increasing the proportion of women in gastroenterology is important for our patients, our practices, and our profession. For many patients, their experience, comfort, overall satisfaction, and adherence to medical therapy all may be improved when they have the option of working with a woman physician. Women tend to seek health care on a more regular basis compared with men and are the health care “executive” for many families because they are the primary managers of children’s care and make most health care decisions for the family. Further, women make 85% of household purchasing decisions, thus commanding significant economic clout and make up one-half of all earners in the United States. In many large metro areas, they are as (or more) educated and earn a higher income compared with their male partners. Thus women as patients, primary caregivers for children and elderly, and earners are key drivers of important health care decisions, including physician selection and management decisions.
Numerous studies have documented women’s preference for the gender of medical providers, particularly when it comes to endoscopy. In fact, some women may decline colonoscopy unless guaranteed a female provider, and this preference may be increasing for office visits as well as endoscopic procedures. We are likely to see such preference trends increase for the following reasons:
- •
The Medicare population will become younger and more diverse as the baby boomer generation ages into Medicare.
- •
Preference for same gender physician increases with younger patient age, current employment, no previous history of colonoscopy, and having a female primary provider.
- •
There are strong gender preferences among certain ethnic and cultural groups and these groups are increasing as a proportion of our practices.
Diversity invites stimulating, creative problem solving and innovation. Workforce diversity thus increases the richness and heuristic range for patient care, practice innovation, and science. The specialty of gastroenterology particularly lends to a collaborative and team-based approach. These are attributes more commonly found among women leaders, who are well-equipped with skills that are widely recognized as requirements for successful leaders: intellectual stimulation, inspiration, participatory decision making, and setting expectations/rewards. Recognizing the leadership potential of women helps to capitalize on the intellectual capacity of our entire workforce.
Women in gastroenterology
The first record of a woman physician dates to about 2730 BC during the reign of a queen in Egypt. Women were included in the famous medical school at Heliopolis and even Cleopatra was trained in the healing arts. Over the ensuing 3 centuries, however, women’s inclusion as medical practitioners grew slowly, impeded by religious and societal prejudices and codified in numerous legal statutes. In the United States, the first woman to earn a medical degree was Elizabeth Blackwell, who graduated from Geneva Medical College in 1849. For those wishing to read personal reflections on the rewards and challenges of women becoming physicians, we refer you to the book This Side of Doctoring: Reflections from Women in Medicine , edited by Chin.
In the last 3 decades, the number of women entering medical school has grown substantially, reflecting a trend in many areas of academia, business, and medicine. In the 1960s, only 5.5% of medical graduates were women but by 2006 that figure had increased to 48.6%. Even though the percentage of women in general internal medicine residencies has increased, women did not pursue subspecialty practice until later, an issue that was emphasized in a 1986 policy paper prepared for the Department of Health and Human Services. Traditionally, procedure-oriented specialties, such as gastroenterology, were male dominated. Inherent training and cultural biases favored men at both the entry point and throughout career advancement. Factors contributing to career barriers for women in gastroenterology are listed in Box 1 .
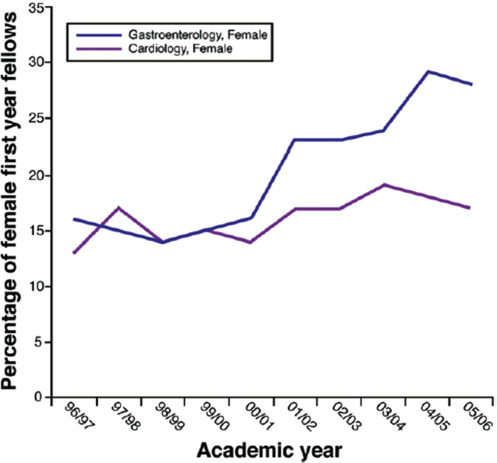
Dr Gail Hecht (the second woman president of the AGA) pointed out, in an editorial published in Gastroenterology , that only 16% of first-year gastroenterology fellows were women in the academic year 1996/1997. In the ensuing decade, the percentage of women in gastroenterology doubled, whereas the percentage of women in another procedure-oriented specialty (cardiology) remained the same ( Fig. 1 ). We believe that this difference reflects the focused efforts of the major gastroenterology societies to recruit women into gastroenterology fellowship positions, despite a shift in the specialty to becoming more procedure dominant.
Although the proportion of women entering subspecialty fields increased, advancing to positions of leadership remained a challenge. As one of this article’s co-authors (CS) stated, “Although the pipeline into our specialty appears robust, like other areas of academia, business and medicine, there has not been a commensurate increase in the proportion of women into positions of seniority, such as advancement into associate or full professor, or into positions of leadership, such as department chair or dean.”
Numerous authors, dating back to the 1970s, have studied the gender bias that occurs in a variety of academic and business careers. Barriers to the ascension of women to leadership positions have collectively been termed the “glass ceiling.” The term “glass” was coined to reflect the subtle and frequently invisible qualities of the barrier; something not rooted in legitimate limitations but rather on discrimination or bias. A clear bias (and one evident in the medical field) is a “status quo bias.” This occurs when companies (or academic departments) are performing well and headed by men. In these situations, there is no perceived need to change the historic pattern of male leadership. Researchers have demonstrated that when male leaders drive a company into crisis, a switch to female leadership often occurs. However, when someone (woman or man) ascends to leadership during a crisis, the chance of failure is high. If the leader in this situation is a woman, companies often remove the new leader and revert to more familiar patterns (male leaders). This phenomenon has been termed “the glass cliff.”
Glass ceilings and glass cliffs have been evident to women gastroenterologists and scientists. We are grateful that a robust pool of excellent women physicians and scientists, with training and accomplishments equal to their male counterparts, now enter our specialty. Yet, we continue to observe a decreasing proportion of women at upper levels of gastroenterology in both private practices and academia. There are few women who lead the large independent gastroenterology groups that now are common in the United States. Similarly, there has not been a comparable increase in women at the level of division or department chair, full professor, or dean.
One measure of academic success is publications, especially in top tier journals. Women’s success in publishing was studied by Long and colleagues and published in Gastrointestinal Endoscopy this year. They found that the proportion of women who are publishing as first or senior authors in the top gastroenterology journals has tripled over the last 20 years, illustrating the fact that gender balance is a recent phenomenon. They also found that women tended to publish in areas of basic science and were less likely to publish endoscopy-related articles. In addition, women tended to publish fewer editorials (usually an invited paper) than would be expected considering the proportion of women in our field. Finally, there were more women first authors when women were in the senior author position, highlighting the importance of mentorship and sponsorship. Jagsi and colleagues noted similar trends when they reviewed women’s contributions to prominent general medical journals. Substantial research indicates that research productivity does not explain differences in career success. Research data such as these will help to inform us about patterns of subtle bias and potentially effective interventions to augment the contribution of women in our field.
Gender equity in digestive disease biomedical sciences has been a topic of publication for years. P. Kay Lund discussed these issues in a 2001 editorial, when she was the lone female associate editor for Gastroenterology . She acknowledged the high representation of women in training and junior faculty positions, but emphasized the disproportionate attrition of women during their ascent to higher ranks. Then, women comprised only 11% of academic professors (data from the Association of American Medical Colleges), 12% of division chiefs, and 7.5% of department chairs. She cited The Project Access study (see reference in the editorial) that showed disparity in career advancement for women in a well-controlled group of matched male and female postdoctoral fellows where neither marriage nor children were statistically different between genders. Other research pointed to gender bias in grant success as well. Lund concluded that a lack of mentoring played a key role in attrition of women from academic ranks, a point she emphasized again in a recent publication. Both Lund and authors Henning and Estes have offered personal hints for women to ponder as they develop a career plan and interact with academic colleagues.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


